German Anguiano Torres रीट्वीट किया

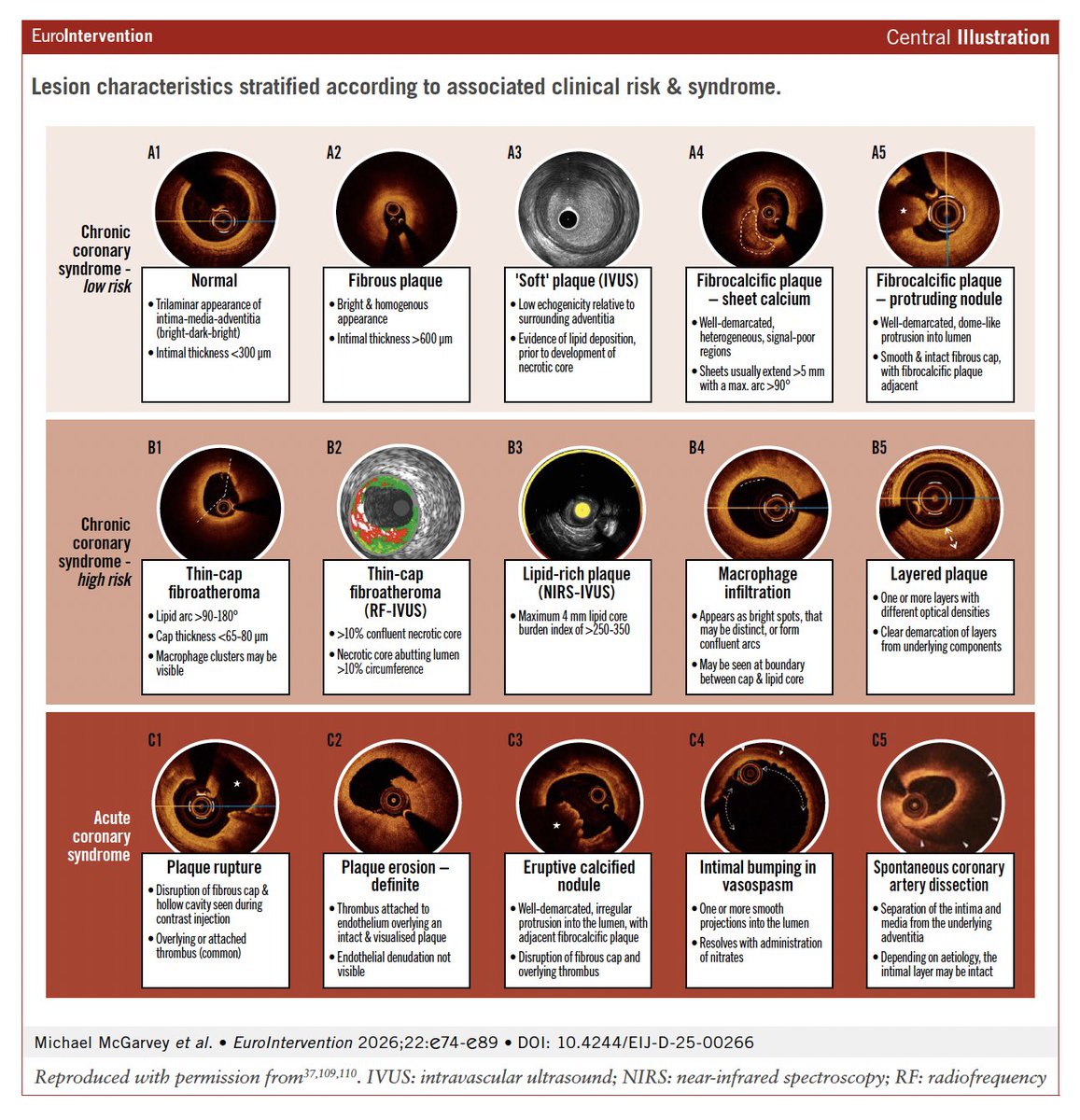
In this new State-of-the-art paper, the authors review the evidence and guideline support for intracoronary imaging in contemporary clinical practice, and outline a modern, imaging-driven approach to PCI planning.
eurointervention.pcronline.com/article/lesion…
English