
JM Tomagan
28K posts

JM Tomagan
@jmtomagan
Radiation Oncologist | Fellow @UTSW_RadOnc | #JRRMMC @USTFMSOfficial Alum | 🇵🇭
Dallas, TX Katılım Ekim 2009
431 Takip Edilen261 Takipçiler
JM Tomagan retweetledi

Incredibly grateful for your mentorship and the opportunity to lead this analysis, @DavidSherMD! These long-term results make a compelling case for the INRT paradigm. Excited for the future of AI-guided precision radiation and HN de-escalation! 📈✨ #ESTRO26 @UTSW_RadOnc
David Sher@DavidSherMD
Absolutely terrific work by @DrSymYoung to report the long-term outcomes of our INRT experience from two prospective trials (INRT-AIR and DARTBOARD). Short version: with long-term follow-up (median 5.2 years for INRT-AIR, 3 years for DARTBOARD), we've seen zero solitary elective nodal recurrences. Longer version: ESTRO has highlighted novel approaches to managing the elective neck in HNSCC, and I believe the future will be very different than the present. Current ENI fields deliver the majority of the integral dose to patients and contribute substantially to critical structures (swallowing and xerostomia OARs). Minimizing ENI dose and volume may meaningfully improve the short- and especially long-term tolerance of radiotherapy. A few more thoughts on our INRT paradigm below:
English
JM Tomagan retweetledi

Absolutely terrific work by @DrSymYoung to report the long-term outcomes of our INRT experience from two prospective trials (INRT-AIR and DARTBOARD).
Short version: with long-term follow-up (median 5.2 years for INRT-AIR, 3 years for DARTBOARD), we've seen zero solitary elective nodal recurrences.
Longer version: ESTRO has highlighted novel approaches to managing the elective neck in HNSCC, and I believe the future will be very different than the present. Current ENI fields deliver the majority of the integral dose to patients and contribute substantially to critical structures (swallowing and xerostomia OARs). Minimizing ENI dose and volume may meaningfully improve the short- and especially long-term tolerance of radiotherapy.
A few more thoughts on our INRT paradigm below:
OncoAlert@OncoAlert
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨 Omission of elective nodal irradiation in HNSCC: long-term results and patient-level pooled analysis from 2 prospective trials (INRT-AIR & DARTBOARD) Presenter Sympascho Young 🇺🇸 A patient-level pooled analysis of 117 patients from two prospective trials (INRT-AIR and DARTBOARD) showed that omission of elective nodal irradiation for HNSCC was oncologically safe long-term, with a 0% rate of solitary elective nodal recurrence at 5 years. The trials used an involved nodal radiotherapy (INRT) approach assisted by an artificial intelligence model for detection of suspicious nodes. @DrSymYoung @DavidSherMD #RadOnc @ESTRO_RT @yasemin09896924 @LindaMrissa @christian_roenn @Valeriadionisi @gerryhanna @clchiang_hk @mtugceyilmaz @B_Tomasik @gmpetrianni @CiroFranzese1 @Atem84 @piet_ost @brachyexpert @BlanceS90 @The_PT_Explorer @BarbaraJereczek @Mat_Guc @ZilliThomas @AnnaKirby17 @PBlanchardMD @achoud72 Pinging OA faculty @MKnoll_MD @_ShankarSiva @Icro_Meattini @seanmmcbride @NiuSanford @nataliagandur @acampsmalea @to_be_elizabeth
English
JM Tomagan retweetledi

APHRODITE is out!
-SIB to mesorectum in early stage rectal cancer increases cCR rate at 6 months (33.3% -> 49.4%) (primary endpoint)
-SIB associated with increase in G2-3 bowel and ano-rectal toxicity.
#ESTRO2026

radoncreview_org@radoncreview
Our “Best of” #ESTRO26 outline is now live! 🚀 What key studies are we missing? Drop any important trials, abstracts, or presentations we should add 👇 bit.ly/BestOfESTRO2026 #RadOnc #ESTRO26 #ESTRO2026
English
JM Tomagan retweetledi
There are tremendous opportunities to improve post-operative radiotherapy in HNSCC. The DIREKHT trial is an excellent example of such work, in which they spared the contralateral neck in a specified group of patients and/or reduced the primary CTV dose to 56 Gy.
The details are important, as over 60% of patients had contralateral (path-negative) neck dissections (from prior publication). Putting aside the controversy of sparing an un-dissected contralateral neck for an oropharynx (non-tonsil) or oral cavity cancer, there is still hesitance to spare a path-negative contralateral neck.
This paper helps assuage those fears. In the original publication, there were 3 contralateral-only LN recurrences, all in un-dissected necks. That means there were zero solitary nodal recurrences in 92 patients with a path-negative contralateral neck dissection, now with long-term follow-up.
If a contralateral neck has been adequately dissected and is negative, it's hard to justify additional treatment to that hemi-neck.
It's difficult to judge the 56 Gy outcomes by abstract alone, especially since the cohort mixed HPV-positive OPC and oral cavity.
Extremely informative trial!
OncoAlert@OncoAlert
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨 De-intensification of postoperative radiotherapy in HNSCC by omitting contralateral elective neck irradiation– long term outcomes of the DIREKHT trial Presented by Charlotte Frei 🇩🇪 #RadOnc ☢️ The DIREKHT trial is a prospective multicentre phase II trial investigating de-intensified risk-adapted radiation in patients with newly diagnosed, non-metastatic HNSCC after surgery. A total of 140 patients were included in the analysis. After five years, overall locoregional recurrence rate was 6.0% (95% CI [1.9; 9.9]). Cumulative incidence of locoregional recurrence was 3.0% (95%-CI [0.1; 5.8]). Details on recurrence patterns and dysphagia rates are presented at ESTRO 2026. @ESTRO_RT @yasemin09896924 @LindaMrissa @christian_roenn @Valeriadionisi @gerryhanna @clchiang_hk @mtugceyilmaz @B_Tomasik @gmpetrianni @CiroFranzese1 @Atem84 @piet_ost @brachyexpert @BlanceS90 @The_PT_Explorer @BarbaraJereczek @Mat_Guc @ZilliThomas @AnnaKirby17 @PBlanchardMD @achoud72 Pinging OA faculty @MKnoll_MD @_ShankarSiva @Icro_Meattini @seanmmcbride @NiuSanford @nataliagandur @acampsmalea @to_be_elizabeth
English
JM Tomagan retweetledi

Two of our faculty, Drs. @MonaArbabMD and Aurelie Garant, along with one of our fellows, Dr. @DrSymYoung, having a great time this weekend at #ESTRO26!

English
JM Tomagan retweetledi

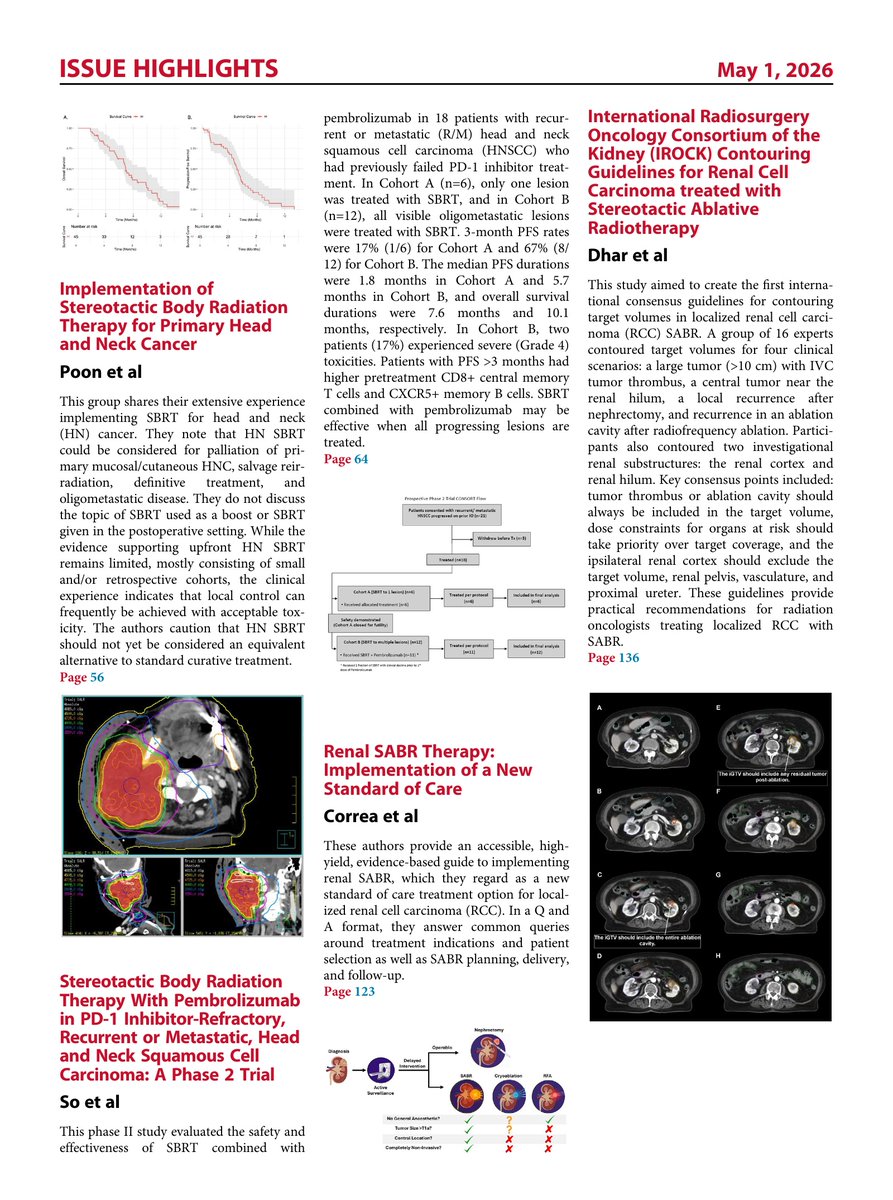
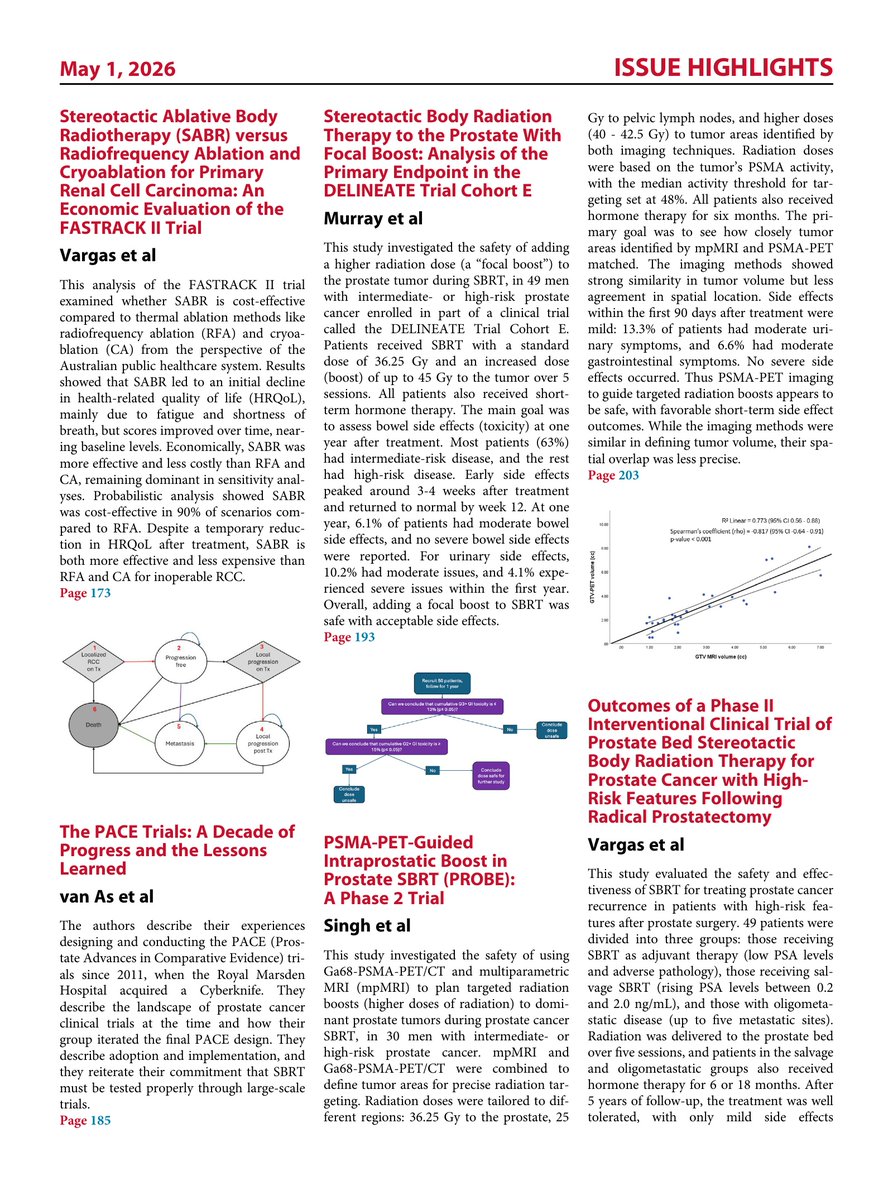
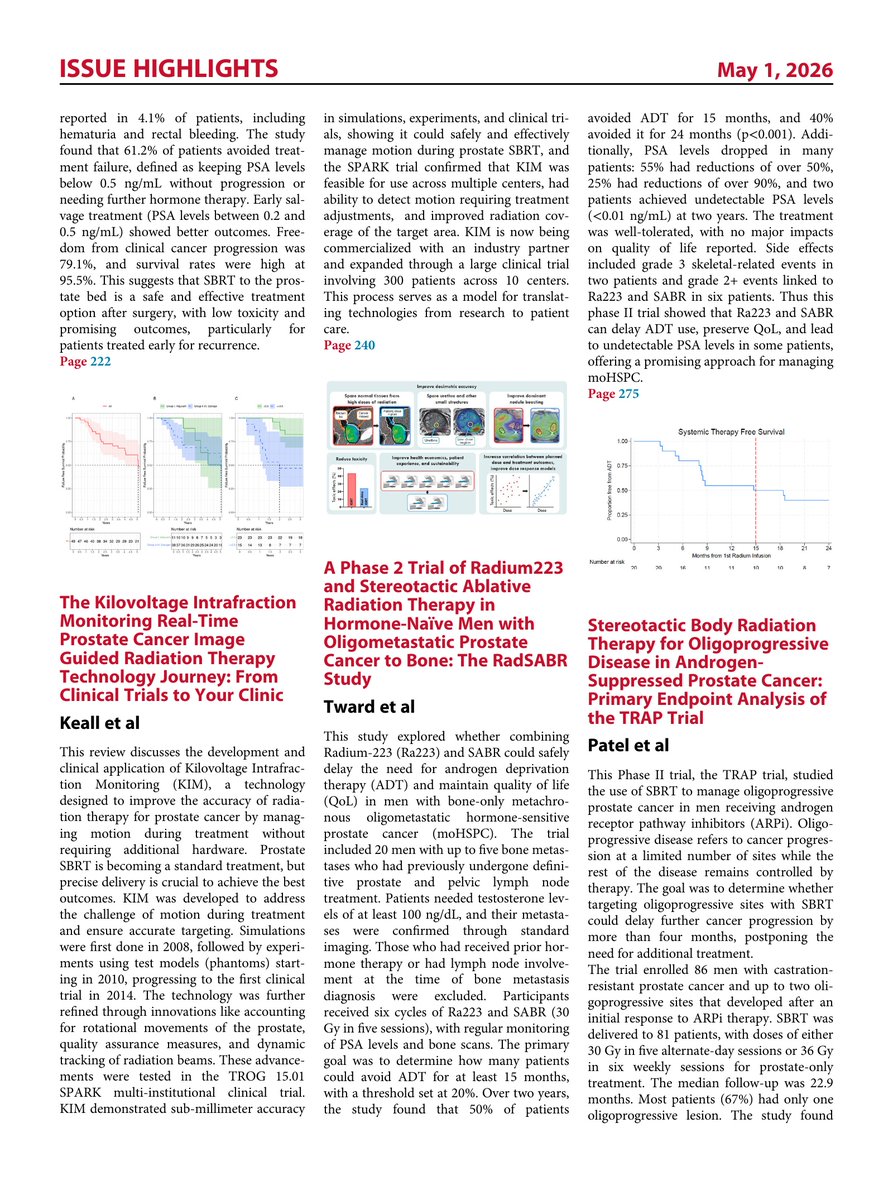
Just released! Volume 2 of SBRT: From Clinical Trials to your Clinic in @IJROBP
Truly amazing papers from end to end. Have a look at the issue highlights here.
redjournal.org/issue/S0360-30…

English
JM Tomagan retweetledi

Studying for Rad Onc Oral Boards? Try out my app Rad Onc Oral Board Sim! It uses AI to generate unique cases and evaluates your spoken responses like a real board examiner. Let me know what you think! #RadOnc #ABR #MedEd
apps.apple.com/us/app/rad-onc…
English
@OncBrothers @BijoyTelivala @RenoHemonc @PTarantinoMD @NVijayvergiaMD @Papa_Heme @ErikaHamilton9 @CathyEngMD @hoperugo @Dr_RShatsky @GIMedOnc Been hearing so much about Open Evidence - need to check it out.
English

A lot of buzz around AI (particularly LLMs). Are you actively using this in your clinical practice?
#OncTiwtter #MedTwitter #HemeTwitter @BijoyTelivala @RenoHemonc @PTarantinoMD @NVijayvergiaMD @Papa_Heme @ErikaHamilton9 @CathyEngMD @hoperugo @Dr_RShatsky @NiuSanford @GIMedOnc
English
JM Tomagan retweetledi
TORPEdO was an incredible effort by the investigators and patients, and the paper analyzes the results extraordinarily well. Given the normalization of outcomes over a very short period of time following treatment, plus the difference in weight loss without any sacrifice in a very low risk of g-tube dependence over time, I agree with the paper’s conclusion: "In health-care settings where IMPT is not used routinely for oropharyngeal squamous cell carcinoma, IMRT remains the standard-of-care.”
Especially since IMRT in 2026 is markedly better than the delivered treatments in the trial, it is hard to see how IMRT shouldn’t always be the standard-of-care.
The key is not stopping there. It is critical to remember that in both arms, about 50% or more of patients reported altered appearance, taste, swallowing and saliva: we need to do better!
And additional improvement clearly will require something more meaningful than protons or photons.
Total dose, elective dose, and elective volumes all need to be personalized and optimized. Let's go!
English
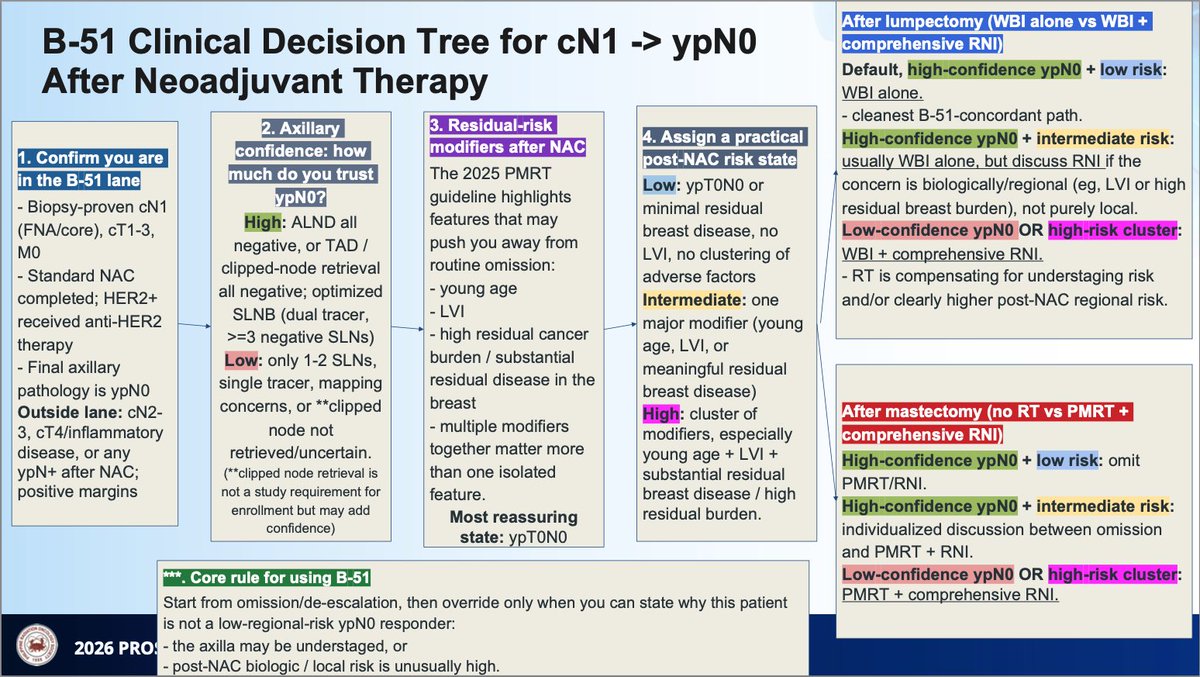
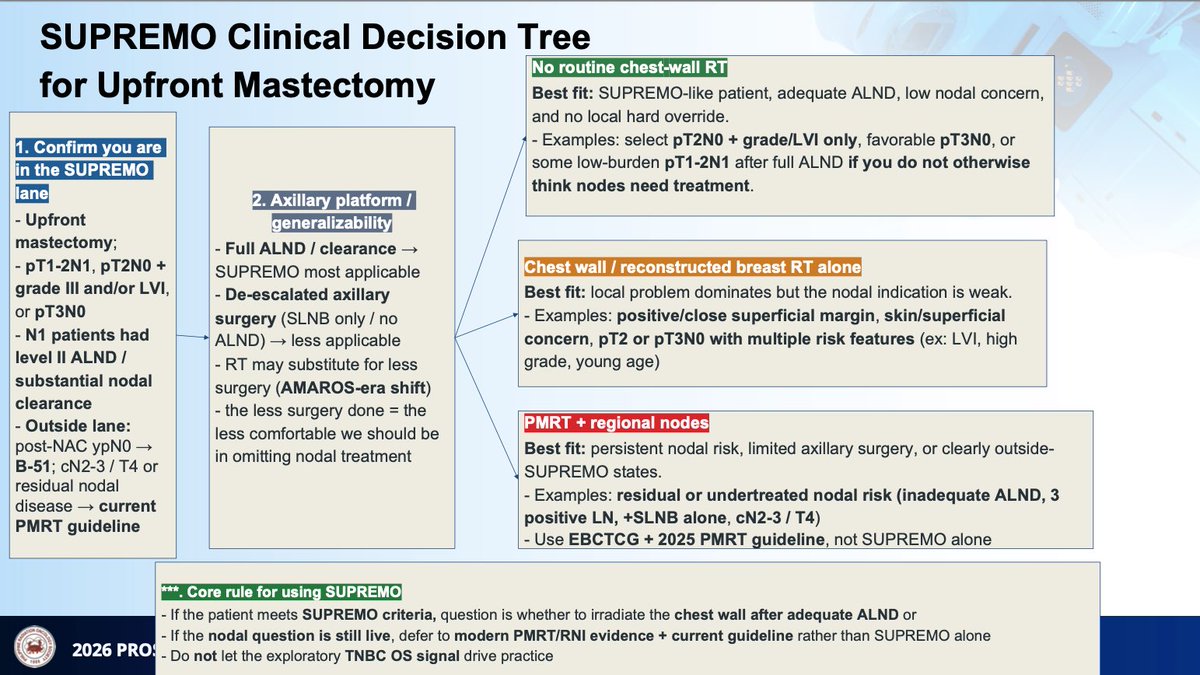
Great decision tree slides by @StephenCiocon at PROS 2026, outlining pathways based on NSABP B-51 and SUPREMO trial.
English
JM Tomagan retweetledi
Callie, a certified therapy dog, stopped by today in her best green outfit and brought smiles to our patients and staff! #HappyStPatricksDay

English
JM Tomagan retweetledi
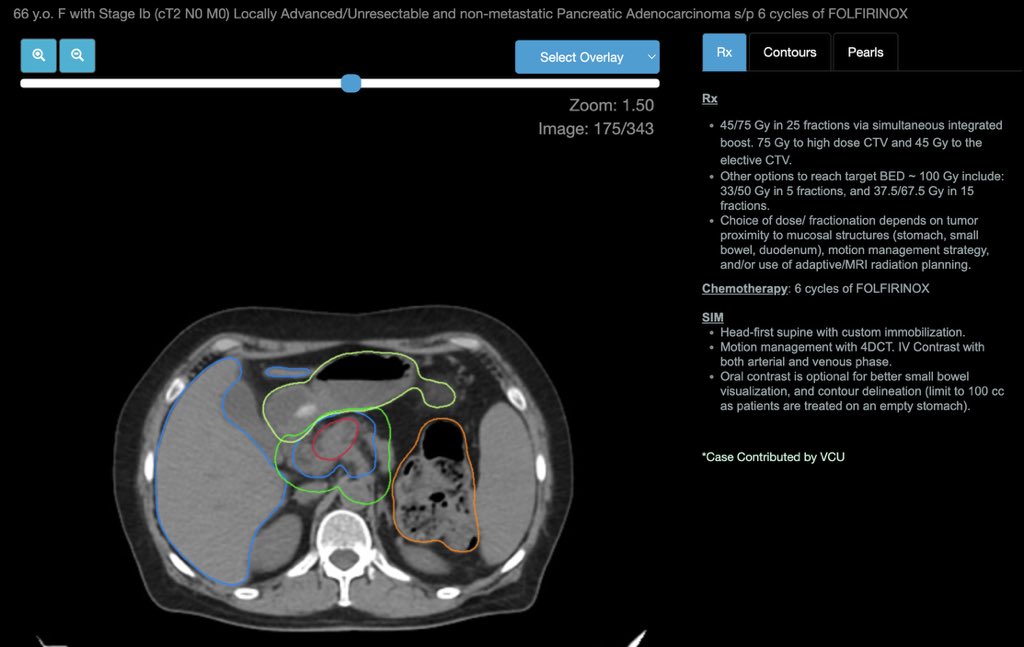
Happy to share this interactive contouring tutorial for dose-escalated RT in locally advanced pancreas ca, which follows our NRG consensus contouring atlas.
Thank you @johnroubil, @dsouzl, @aiims2738, & the @eContourRadOnc team for working on this case!
econtour.org/cases/180
English
JM Tomagan retweetledi

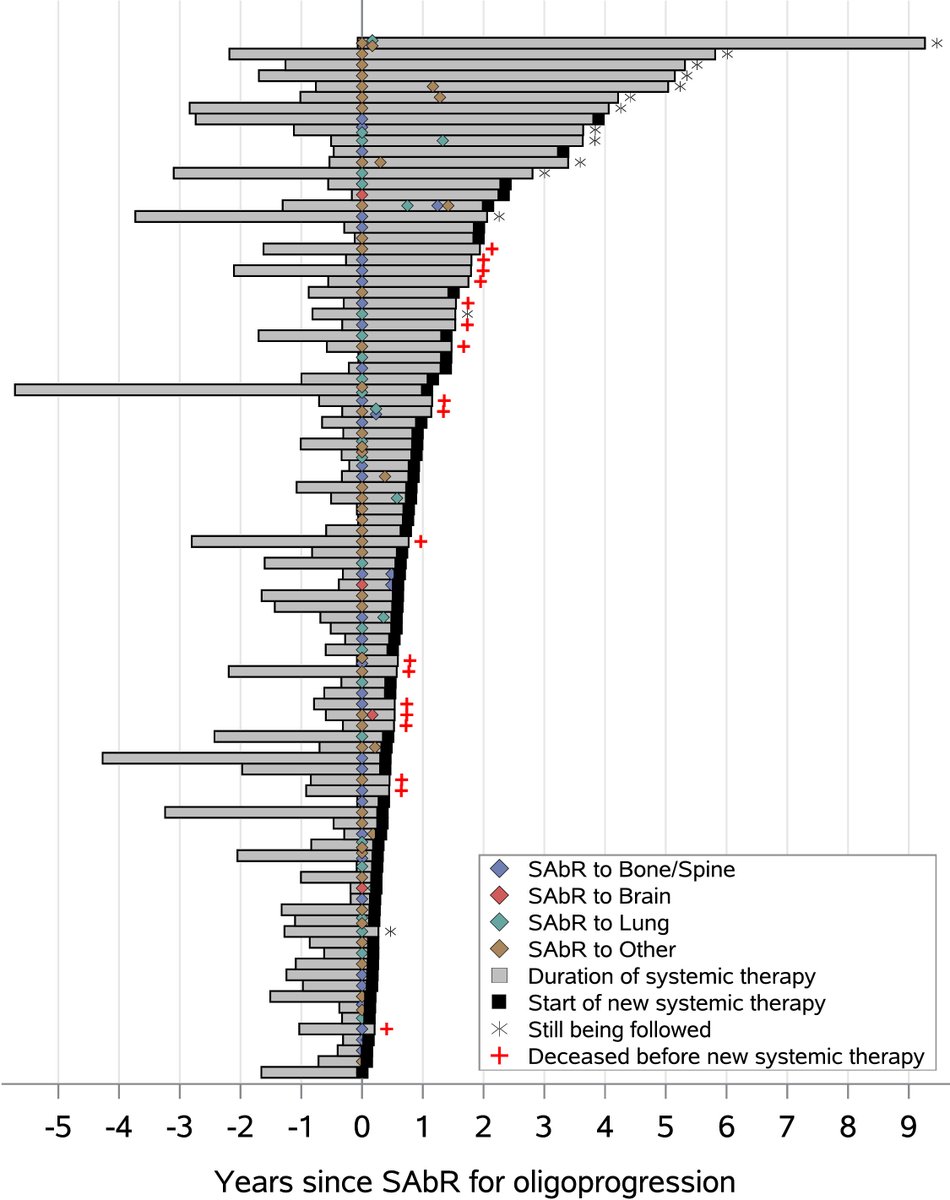
New from @Raquib_Hannan in the #RedJournal: One of the largest cohorts of oligoprogressive #RCC treated with #SAbR during systemic therapy. tinyurl.com/rjlzhao
English
JM Tomagan retweetledi
I’ve been looking forward to this paper since the ASTRO Plenary talk in 2023.
HYPNO-RT is out: is it worth the wait?
redjournal.org/article/S0360-…
English
JM Tomagan retweetledi
Explore the latest in adaptive radiotherapy (ART), from current clinical applications to AI-driven innovations during our ART Symposium! We will have several expert speakers discussing the latest advancements in ART.
🗓️: April 16-17
Register here ➡️: bit.ly/4pAWtIc


English
JM Tomagan retweetledi


JM Tomagan retweetledi
A few thoughts on our experience in this oligometastatic endeavor:
- Some patients had a difficult time with randomization to a less aggressive arm. Despite the possibility of salvage SBRT or HN radiotherapy at recurrence, the successful prior history of local consolidative therapy (LCT) made it difficult to accept systemic therapy alone.
- It is challenging to open a cooperative group trial (with little financial benefit) that has a limited patient population. On one hand, only coop trials can answer such a question, but on the other, institutions’ research operations are struggling to stay afloat and are very strategic with what trials they open. We tried to open EA3211 to a wider patient population but didn’t have enough runway to show accrual was feasible with our new criteria.
- In the first-line setting, there are many, many competing systemic therapy trials that pay sites (much) more money per patient and offer the hope of “better" immunotherapy. Especially in this financial environment, it is tough to compete with money.
- However, I also think there is a profound under-appreciation of both the benefit of LCT given its typically modest toxicity and the potential high-grade toxicity of novel systemic therapies. Drugs can cause real harm, and gross disease is the most likely metastatic deposit to recur.
- As we think of new trials in this space, we need to stratify the metastatic population (notice, I did not focus on just OMD) into very distinct cohorts that may benefit from SBRT and other forms of LCT (surgery included). The EORTC formalism is wonderful but complicated (sciencedirect.com/science/articl…), so this approach below (for the sake of discussion on trial concepts) is simplified.
- There are patients with previously untreated de novo disease, who have both primary and metastatic cancer. A critical question is whether we should treat the primary, both to prevent primary progression and its morbidity/mortality and potentially a main source of further metastatic spread. Such treatment can cause acute morbidity but may have the highest yield as a radiotherapy intervention. There are some trials looking at this question, and the benefit likely will profoundly vary by primary site. We included this population in EA3211, but it was too rare to push the trial forward.
- In this same population of previously untreated cancer, managing the metastatic disease is basically a separate question. Here the morbidity of SBRT is much less, and just irradiating each deposit may perform plastic surgery on the scans (saw that language on a previous X discussion) without a long-term clinical benefit, especially since progression is almost always radiographically-detected. I would argue that OS is still the relevant endpoint since salvage SBRT is typically still feasible and efficacious; PFS will make us feel good but not move the needle on more patients living or feeling better. I sincerely hope that we can complete trials in this space, but as we have seen in EA3211, it’s quite tough for the reasons mentioned above.
- In a population that clearly needs systemic treatment, it is absolutely imperative to identify biomarkers (both circulating and radiographic) to distill out patients with detectable (i.e. consider LCT) versus non-detectable disease/MRD. It takes money and collaboration (to generate enough data), but such work (to identify an integral biomarker) is probably the sine qua non of OMD treatment in these patients. The NCI may pay for an integral biomarker in a trial but typically not the research needed to identify one.
- There is a second cohort of patients with previously treated localized disease who now present with new metastases. This group formed the bulk of EA3211 and is probably the most common group of individuals for whom we consider LCT to metastatic disease. To some extent it depends on the time to develop metastases, but here I think we need to focus on a different question than systemic therapy +/- LCT. Patients (and physicians!) may not accept this randomization, competing systemic therapy trials may feel more compelling, and salvage to radiographically-detected progressive mets is feasible (see above). These patients probably need two arms that possess distinctly differently therapeutic approaches.
- Especially in this era of IO (and a few other targeted therapies) that can lead to long-term disease control but with significant toxicities, we should focus more trials on LCT versus systemic therapy (like the HN OMET trial and several efforts in renal cell). Can LCT delay (or prevent) the need to start systemic therapy in a meaningful number of patients? I have had several patients with biopsy-proven metastatic disease cured with LCT, not to mention the group whose systemic treatment was meaningfully delayed. Generally speaking, SBRT is much easier to tolerate than systemic therapy, and this comparison (LCT vs systemic treatment) has many important endpoints, including QoL/PRO and the potential to delay systemic therapy without compromising survival. It will take a change in mindset (mostly among our medical oncology friends) to offer a trial in which patients are not receiving upfront systemic therapy, but personally I feel like this is the way in this cohort.
- There is a final, substantial cohort of patients with growing (or perhaps persistent) metastatic disease despite systemic therapy, where the typical non-LCT approach is second-line therapy. Here is a fantastic opportunity for LCT to show its utility, either from a survival standpoint or by delaying typically less effective and/or more toxic second-line treatment. There is a wonderful recent editorial on relevant, patient-centered endpoints (t.co/TH7FHQhYnd). This oligoprogressive space may be the sweet spot for further trials; the alternative is suboptimal, but the clinical gain needs to be established.
- The forever question of “what is oligometastatic?” is not easy to answer, and the needle is constantly moving and being tested. In EA3211, we used 4 isocenters as the threshold, which was meant to be practical and allow a pretty generous number of metastases (esp in the mediastinum). Personally I believe this is a biological rather than radiologic issue, but we just need to see the results of trials in this space to better understand the possibilities and therapeutic ratios of different SBRT schemes and doses (optimal dose is a whole separate question).
English
JM Tomagan retweetledi
Given the recent discussions on novel radiotherapy approaches in H&N radiotherapy, it is a great time to discuss our @UTSW_RadOnc DARTBOARD study, which is available in @JNCI_Now!
academic.oup.com/jnci/article-a…
English
JM Tomagan retweetledi
This symposium is going to be tremendous.
There will be experts in x-ray and MR-based adaptive radiotherapy, covering *multiple* vendors, and there will be presentations on both the current state and future vision of adaptive radiotherapy.
Speakers are coming from all over the world!
We prefer to meet you in-person, but a virtual option is available too.
Please consider coming to Dallas in April (weather is fantastic this time of year, and I can't say that very often)!
UTSW Radiation Oncology@UTSW_RadOnc
Registration for our ART Symposium is now open! Explore the latest in adaptive radiotherapy, from current clinical applications to AI-driven innovations. Open to radoncs, physicists, dosimetrists, therapists, and more. Learn more and register here ➡️: bit.ly/4pAWtIc
English