Rodrigo Aranibar Martinez retweetledi

🚨JACC Focus Seminar: complicaciones mecánicas del IAM. 🫀💥🔥
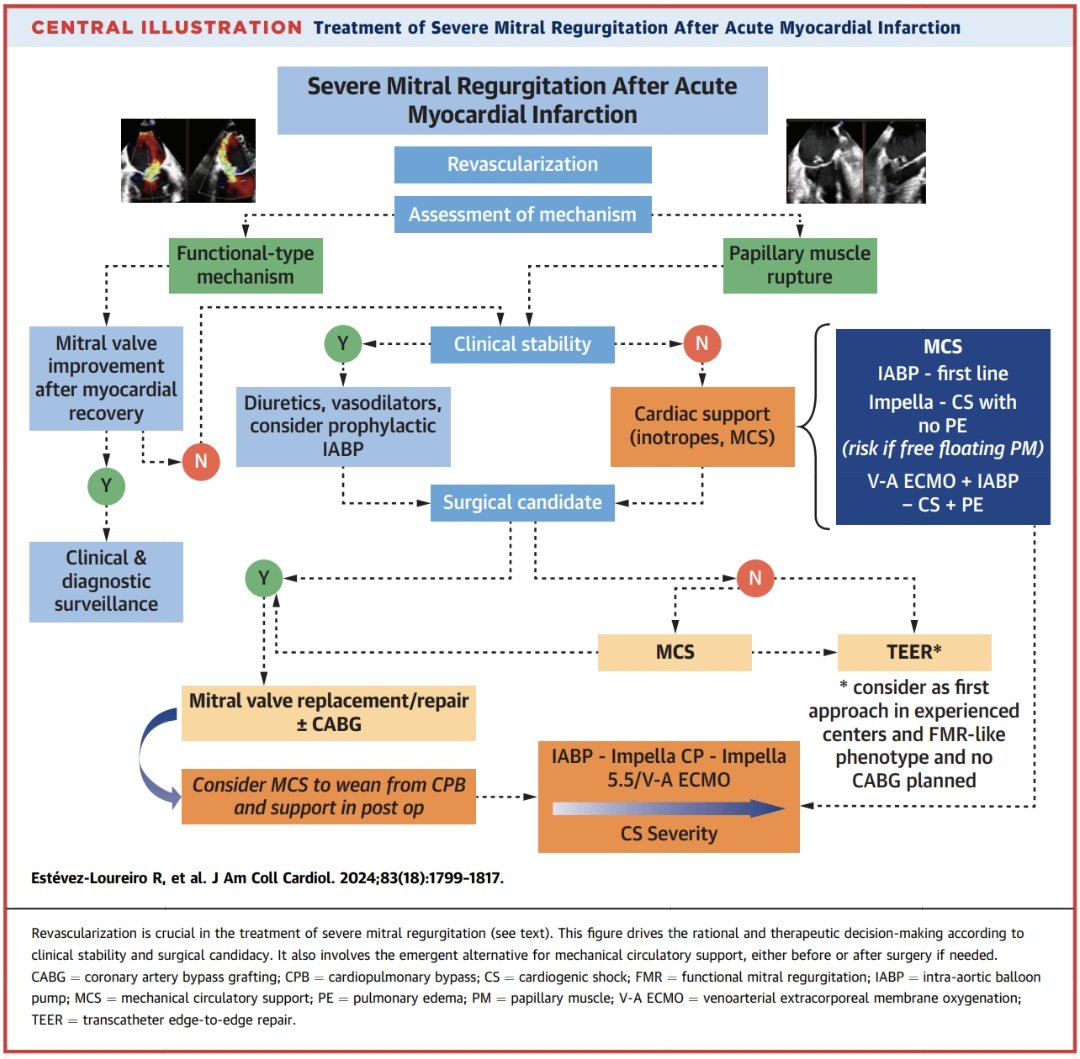
🔹Insuficiencia mitral aguda post-IAM: generalmente secundaria a ruptura del músculo papilar. Produce edema pulmonar y choque cardiogénico rápidamente. La cirugía sigue siendo el estándar, pero el soporte mecánico temprano (Impella/ECMO) y el TEER tipo MitraClip emergen como alternativas en pacientes de alto riesgo.
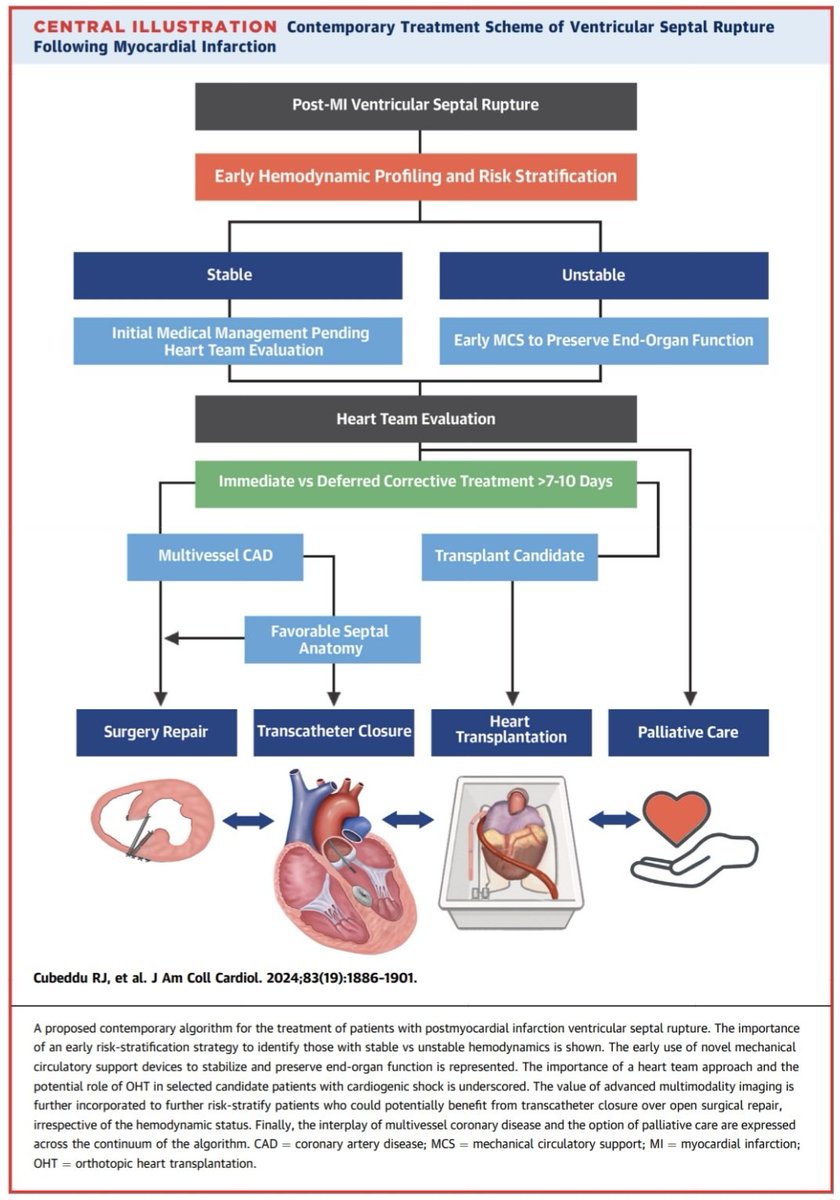
🔹Ruptura del septum interventricular (CIV postinfarto): complicación devastadora con cortocircuito izquierda-derecha y colapso hemodinámico. El Eco Doppler es clave. La estabilización con soporte circulatorio antes de cirugía puede mejorar supervivencia. El cierre percutáneo se considera en casos seleccionados.
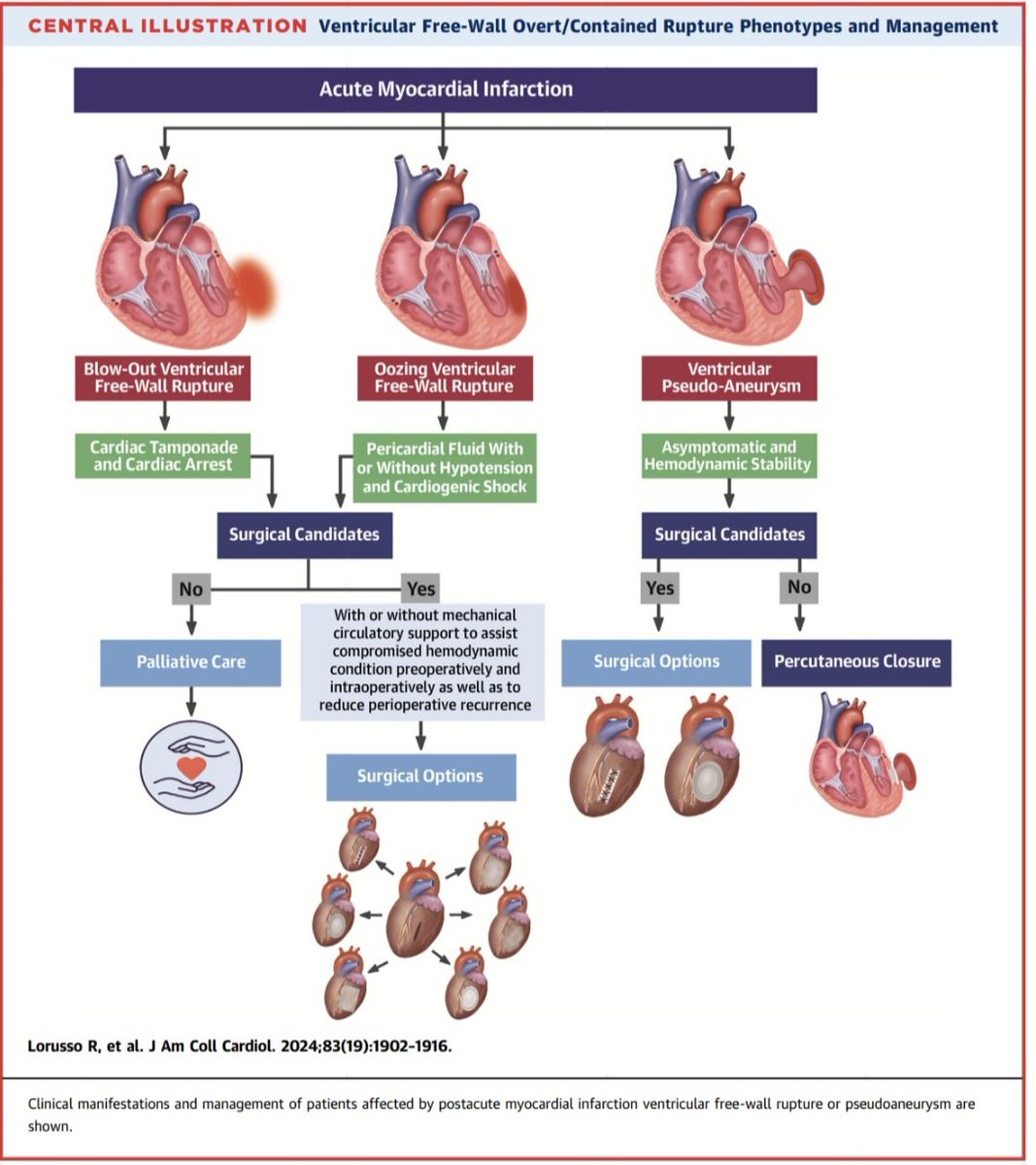
🔹Ruptura de pared libre y pseudoaneurisma: la ruptura libre suele causar taponamiento y muerte súbita. Cuando la ruptura es contenida se forma un pseudoaneurisma, con alto riesgo de ruptura posterior. La imagen multimodal (eco, TC, RM) es fundamental para diferenciarlo de aneurisma verdadero y planear tratamiento.
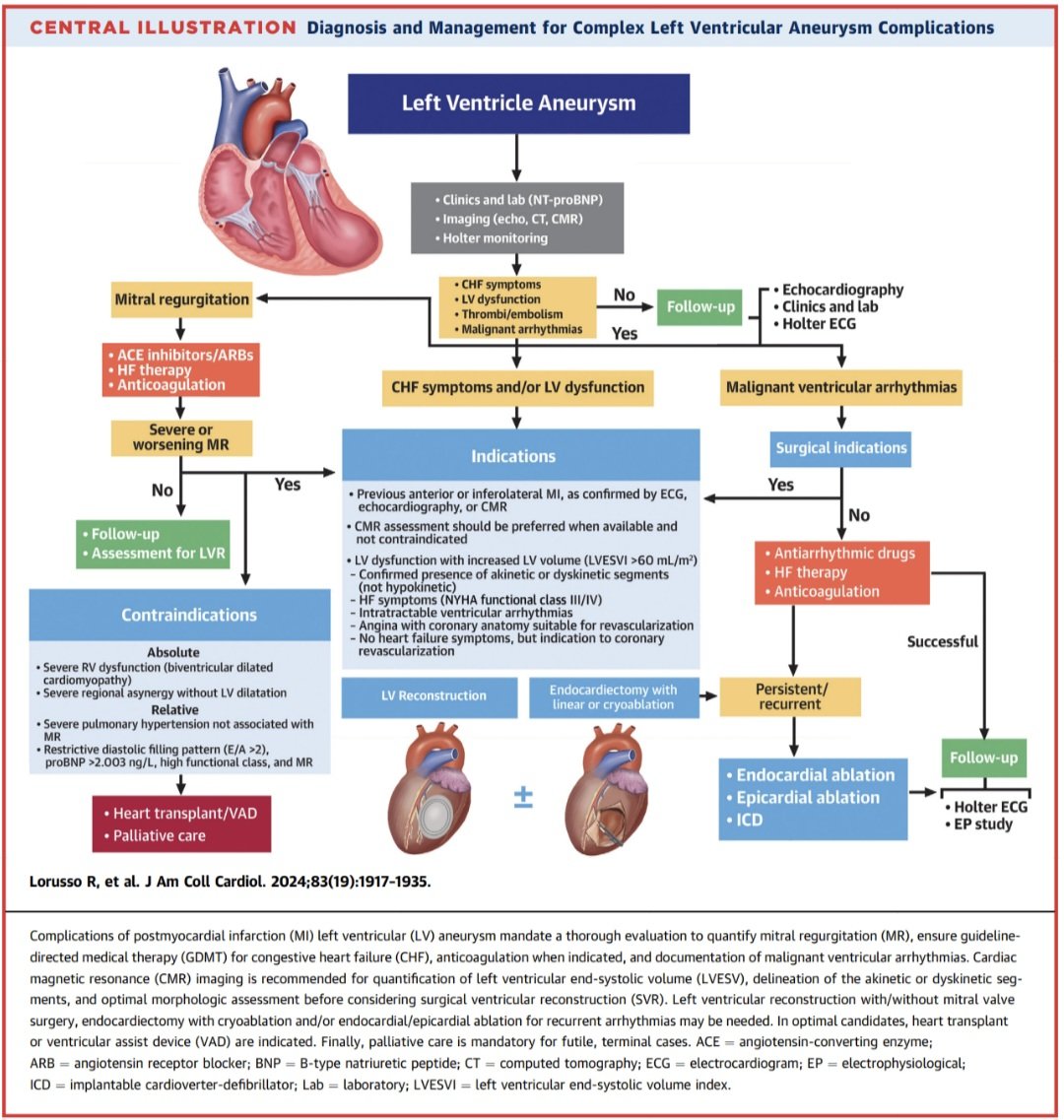
🔹Aneurisma ventricular: secuela tardía del IAM transmural. Puede causar insuficiencia cardiaca, trombos, embolias y taquicardia ventricular. El manejo incluye terapia médica, anticoagulación, DAI y en algunos casos reconstrucción quirúrgica ventricular.
📜🆓️⤵️
t.me/medicinaintern…
Español