@PTarantinoMD What are your thoughts on the usage of nab paclitaxel in Neocarhp? Does it add any value?
English
Dr Arun Chandran
213 posts

@groundhogcs
Medical oncologist / theoncodoctor!/

















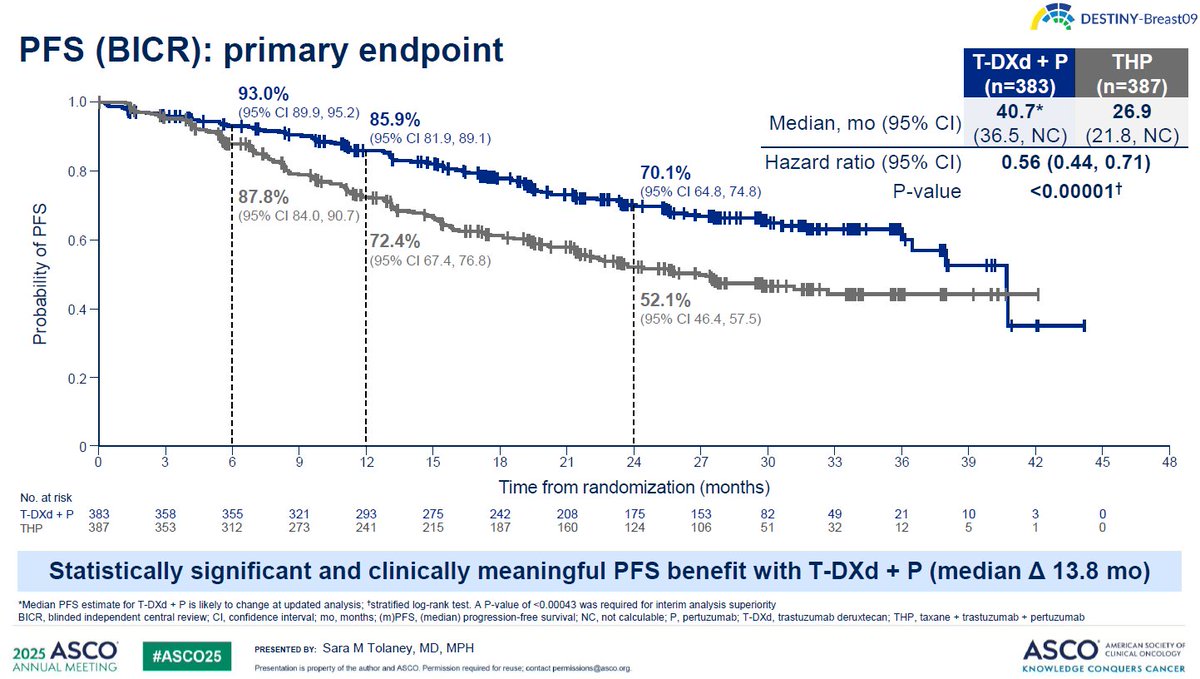
Great news💫 T-DXd plus pertuzumab has been approved by the FDA as a first-line treatment for HER2-positive mBC