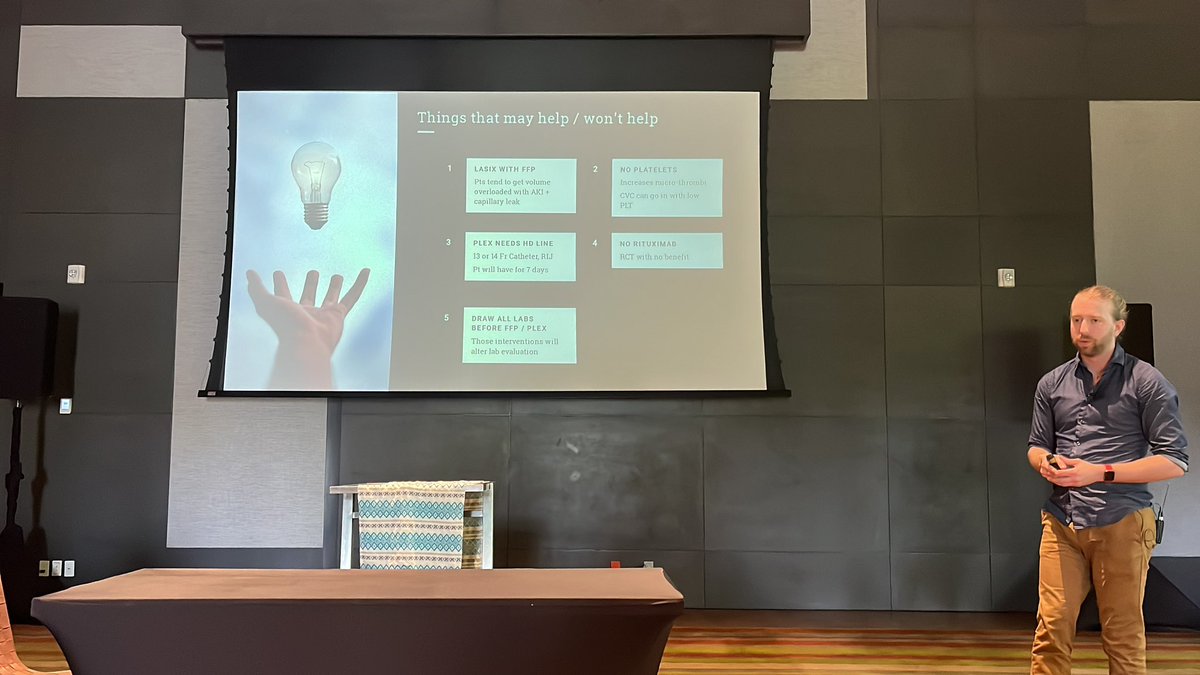
@srrezaie discussion about Andexanet alfa and it’s use in ICH #resusxreunion2024
Always triple check big Pharma funded studies!! The primary outcome was hemolytic efficacy butshowed increased thrombotic events!!
GIF

English
Dr Dee Sanchez
1.3K posts

@DeeOptimal
MD, MIS, PMP, NREMT, NASM-CPT, FAWM Candidate | EM PGY1| IG= @drdee2022 | Passions: #wildernessmed #medinformatics #ems #emergencymed #tweetsnotmedicaladvice