Hot flushes, previous breast cancer ….Veoza now funded by NHS

English
Rick Linforth
3.7K posts

@RICKLIN4TH
Consultant Oncoplastic Breast Surgeon Surgical Innovator and National trainer for Association of Breast Surgery.Medico-legal expert,BWFC fan.


High quality RWD to fill a relevant evidence gap: among 501 young (≤40) pts with node-positive, ER+ breast cancer who had received 5y of OFS, extending ET beyond year 5 was associated with better IBCFS & DRFS. Led by super @ValenzaCarmine! @DFCI_BreastOnc ascopubs.org/doi/10.1200/JC…






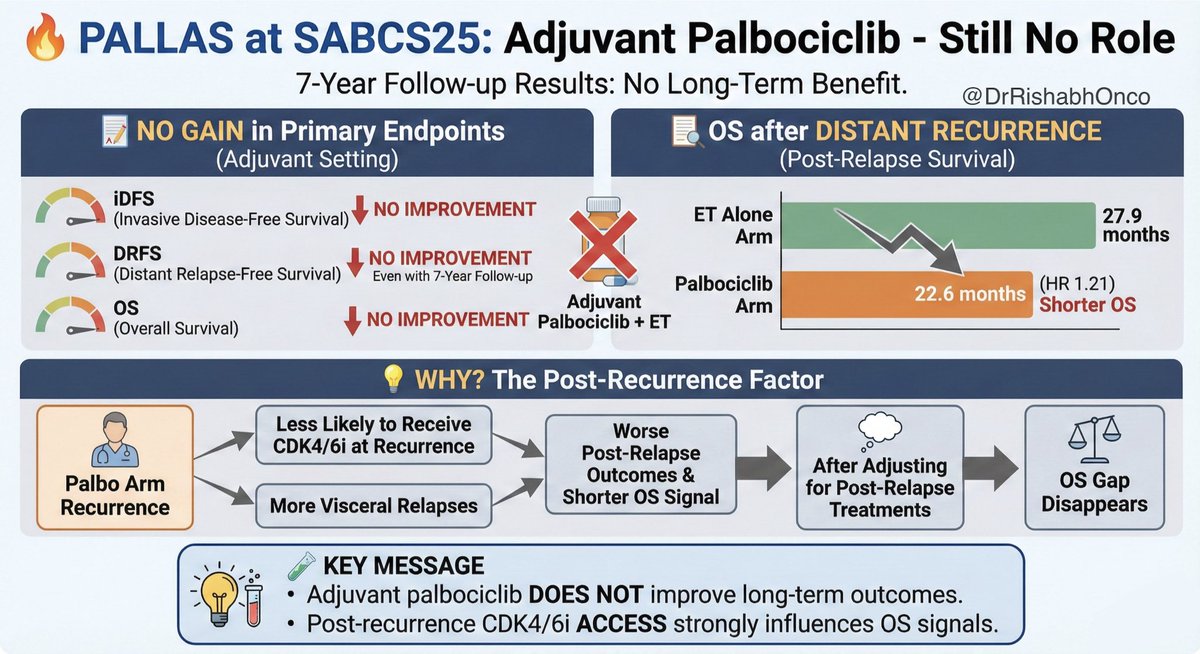
🔥 PALLAS at #SABCS25 : Still no role for adjuvant Palbociclib Even with 7 year follow up, PALLAS again shows no gain in iDFS, DRFS, or OS with adjuvant palbociclib. 📉 OS after distant recurrence Shorter in the palbo arm: 22.6 mo vs 27.9 mo for ET alone (HR 1.21). 💡 Why? Palbo patients were less likely to receive CDK4/6i at recurrence and had more visceral relapses, pushing outcomes down. After adjusting for post relapse treatments, the OS gap disappears. 🧪 Key message Adjuvant palbociclib does not improve long term outcomes. Post recurrence CDK4/6 access strongly influences OS signals. #OncoTwitter #MedTwitter #BreastCancer #SABCS25 @OncoAlert @myesmo @esmo_open @ASCO

Tamoxifen in the absence of definitive surgery for low risk DCIS was associated with an unacceptably high risk of invasive breast cancer 10% at 5 years exceeding planned limit of risk. Bottom line: DCIS still warrants surgery @SABCSSanAntonio #SABCS25

Less can be more in the axilla at #SABCS25 💡🫁 New #AXSANA data shows that for patients converting from cN1 to ypN0 after NACT, SLNB or TAD matches ALND for 3 year axillary control. Almost zero difference in recurrence. Almost zero reason to overtreat. ➡️ 3 year axillary recurrence free survival SLNB 99.8 percent TAD 98.5 percent ALND 99.2 percent (All confidence intervals overlapping) ➡️ Key message More surgery did not translate into more regional control. Axillary management can be safely de escalated in ycN0 after NACT, provided standards are met. 💭 Why it matters? Avoiding ALND means fewer complications, better QoL, and similar oncologic outcomes. #OncoTwitter #MedTwitter #BreastCancer #SABCS25 @OncoAlert @myesmo @esmo_open @asco