Tweet fijado
Dr Divago
287.4K posts

Dr Divago
@DivagoTM
stabbing people to life https://t.co/H8oflJaaNS
Se unió Nisan 2012
1.6K Siguiendo12.9K Seguidores
Dr Divago retuiteado


@Eduardoigbrasil @seilatopistolaa @medicomunista_ Top 10 momentos vividos foi quando meu colega de R2 pegou o eletro da mão da especializada de CM e virou de cabeça pra cima.
Português

GIF
Português
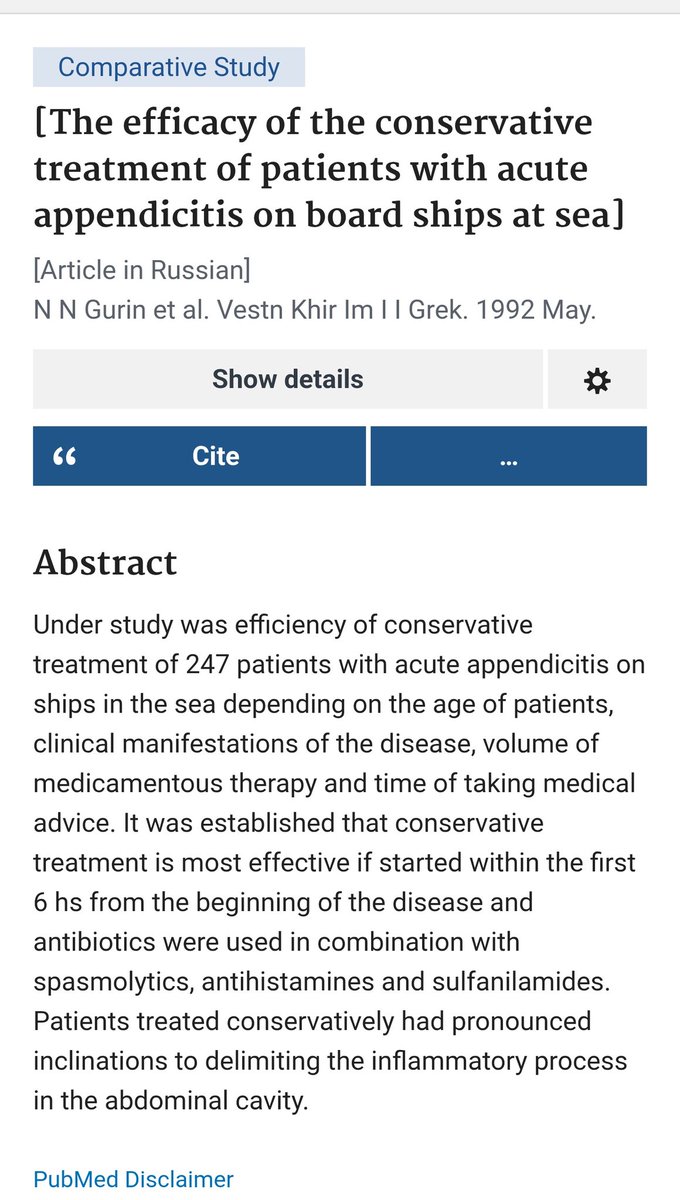
@rbarbosa91 @jdimick1 @ZhiVenFongMD It was all the rage in the Russian fishing boats in the 80s... Useful to get you to firm land, no reports - that I know of - on the recurrence rates they had as the goal wasn't definitive management, it was just "management".
English

@DivagoTM @jdimick1 @ZhiVenFongMD NOM makes sense in certain situations (frailty, hostile abdomen, etc.) though not for everyday routine management. I had one mild case where the patient was about 4 hr away from a flight home to the East Coast, and I said yeah, Abx will get you home and you can decide there.
English
Dr Divago retuiteado

The framing for this has always seemed strange to me.
Surgery has a 0% failure rate at preventing recurrent appendicitis (yes if done well) and antibiotics a 44% failure rate.
Unless surgery is strongly contraindicated, appendectomy seems like the right choice.
JAMA@JAMA_current
In adults with uncomplicated #appendicitis, 44% treated with antibiotics required appendectomy within 10 years, but complication rates were lower and quality of life similar to surgery. ja.ma/3NU446Z
English

And I don't know how you do it
Making love
Out of nothing, et al.
Jason, ex Inferis@benedictsred
Nothing stopping us from changing “et al” to “and the fellas”
Ireland 🇮🇪 English
@DermatoBarbie @lourentuza Teve um na mídia até recente não teve? Pessoal nunca aprende
Português

@lourentuza o TANTO de creme anestésico
a desquerida correndo risco de ir de arrasta
Español

É impossível fechar as costas com um trabalho foda em uma sessão só! Falei “trabalho foda” não essa nojeira ai!
Lucas 🦇@vlucasrocha
e essa mulher que decidiu fechar as costas com uma tatuagem numa única sessão
Português
Dr Divago retuiteado

I don't know whether you guys are history buffs, but this is quite a turnabout for both parties
The Kobeissi Letter@KobeissiLetter
BREAKING: Volkswagen is in talks with Israel’s Iron Dome maker over a deal that would switch production at one of their factories from cars to missile defense, per FT. The German government is actively supporting the proposal.
English
@medicomunista_ @seilatopistolaa @Eduardoigbrasil Veja bem o maior motivador pra um cirurgião saber clínica médica é pra oportunidade de desmerecer um clínico que saiba menos que ele
Português
@seilatopistolaa @DivagoTM @Eduardoigbrasil no máximo tu vai ver um paciente constipado que te mandaram pensando que era abdome agudo cirúrgico mas na vdd era hipoNa e aí você vai mandar de volta pra clínica médica. essa é a meta

Português
Português
@seilatopistolaa @DivagoTM @Eduardoigbrasil meu sonho chegar na fase em que distúrbios do sódio não vão ser problema meu mais

Português
Português

@medicomunista_ @Eduardoigbrasil @DivagoTM pior q um chefe ja comentou uma vez sobre isso e fiquei convencida do mecanismo tb mas fico mt cetica ainda parece mt errado
Português
@rbarbosa91 @jdimick1 @ZhiVenFongMD Every now and again I'm faced with a very mild appendicitis in a very - otherwise - sick patient. Poor anaesthetic candidate, socially in a difficult situation, etc. I've been happy to, exceptionally, use the NOM option in those cases.
English
@jdimick1 @ZhiVenFongMD IMO there seem to be 2 ‘nonop’ camps with different motivations:
Camp 1: academics that want papers
Camp 2: systems that struggle to meet the existing workload, and need to decrease it somehow. If they can get rid of appendectomies, it would make a difference for them.
English

@DivagoTM Penso a mesma coisa que você! Sei que vou ganhar menos mas jamais quero ficar o resto da vida como generalista ganhando mais, me matando e infeliz. Afinal, eu não estou fazendo pediatria por dinheiro, né? Kkkkkkkk Só achei engraçado o comentário dela, pqp! É foda.
Português
Hoje uma interna disse assim: ai pra que fazer uma residência se vai ganhar menos que um generalista depois?
Me atacou por que?????
Português
@jdimick1 @GI_Pearls Not to say that, albeit all biased in selection, follow up etc, we should be doing better than Russian fisherman at sea in the 1980s by now
Ireland 🇮🇪 English
@biasoprolol Caiu demais qualidade esse ano, tão praticamente dando os ovos de páscoa deles e ninguém quer
Português

Roubando nossas pautas como roubaram nosso ouro
Rt Hon. Will || Portfolio for Sarcasm (parody)@colder_sarcasm
I’m absolutely outraged!!! I’ve just found out that Cadbury are flattening Easter Eggs into some kind of bar and are selling them all year round in a further attack on Easter!! We are a Christian country!!
Dublin City, Ireland 🇮🇪 Português

@mirimemiri Na BBC antigamente os caras sempre que mensagens uma marca (sei lá, coca cola) eles precisavam dizer "other brands are also available" pra não ficar subentendido que eles estavam promovendo o uso daquela marca específica.
Talvez isso seja necessário no Twitter hoje em dia
Português

aqui nesse site se você comenta uma característica de A sem obrigatoriamente citar também a opção B as pessoas assumem automaticamente que você É CONTRA B
é realmente o lugar onde a nuance vem pra morrer
Português