
Ankur Singh, DNB (Path) retweetledi

Biallelic TP53 loss is NOT included in IMS/IMWG 2024 risk stratification.
Yet most would agree: this is ULTRA –High RISK myeloma.
WHY ? Because we only include what we can measure.
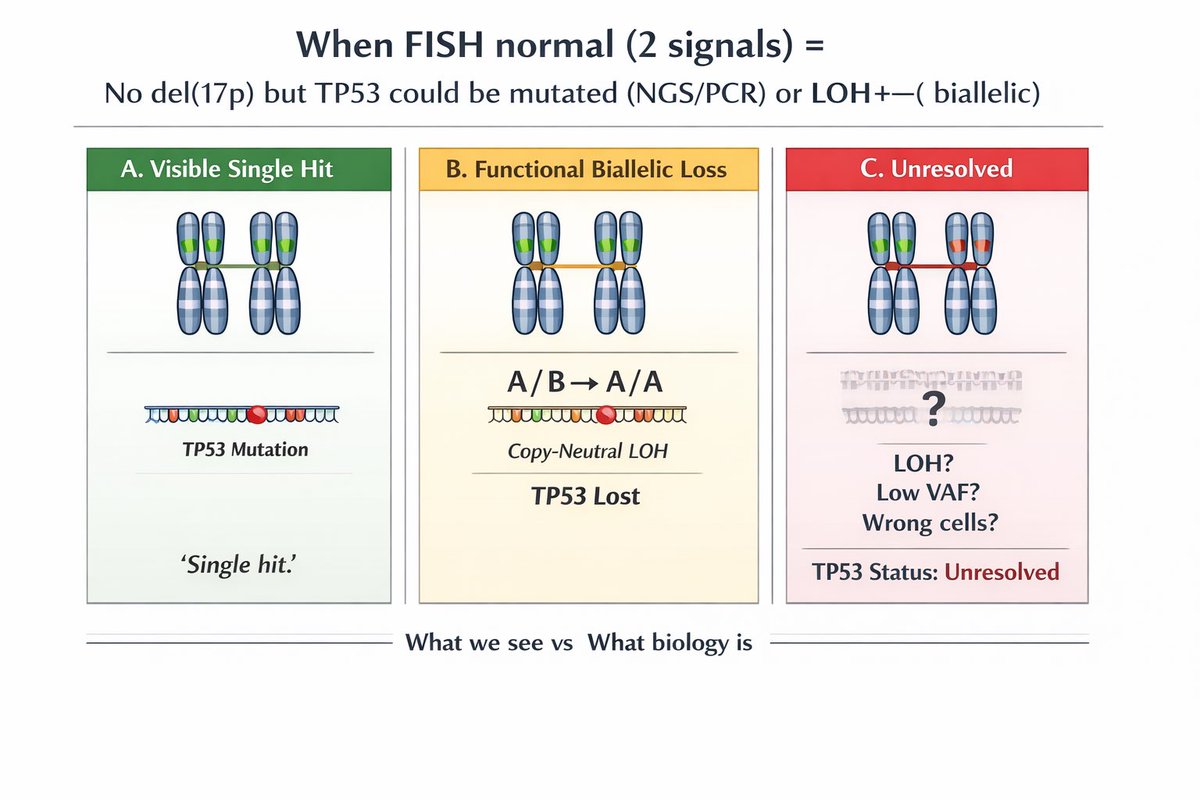
FISH detects del(17p) → only one hit
NGS detects mutation → may suggest double hit but misses many
VAF >60% is suggestive, not confirmatory
CMA/SNP is key:
• Detects copy-neutral LOH
• Mutant allele duplicates, wild-type lost
• True biallelic inactivation
We measure deletions… BUT biology operates through loss of function.
Bottom line:
FISH + NGS + CMA are needed for full TP53 assessment
Until then, we are under-calling ultra–high risk myeloma.
#myeloma #MultipleMyeloma #Hemetwitter #smmm

English