
Dr Pakyto
2.4K posts

Dr Pakyto
@DPakyto
Since the Time of John the Baptist, the Kingdom of Heaven Suffers Violence and Only the Violent Take it Away...
Hospital General de Mexico Entrou em Kasım 2020
981 Seguindo122 Seguidores


Dr Pakyto retweetou

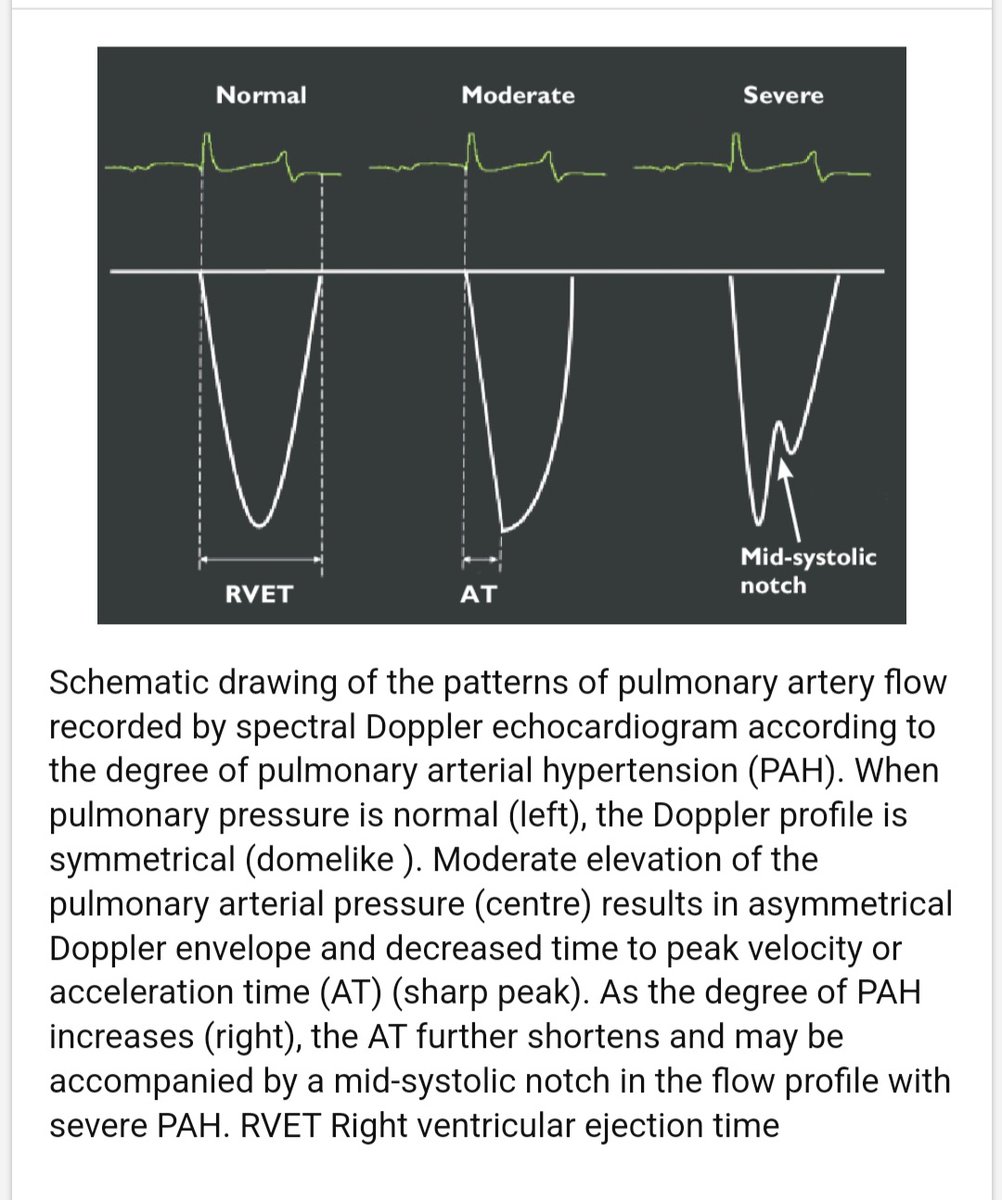
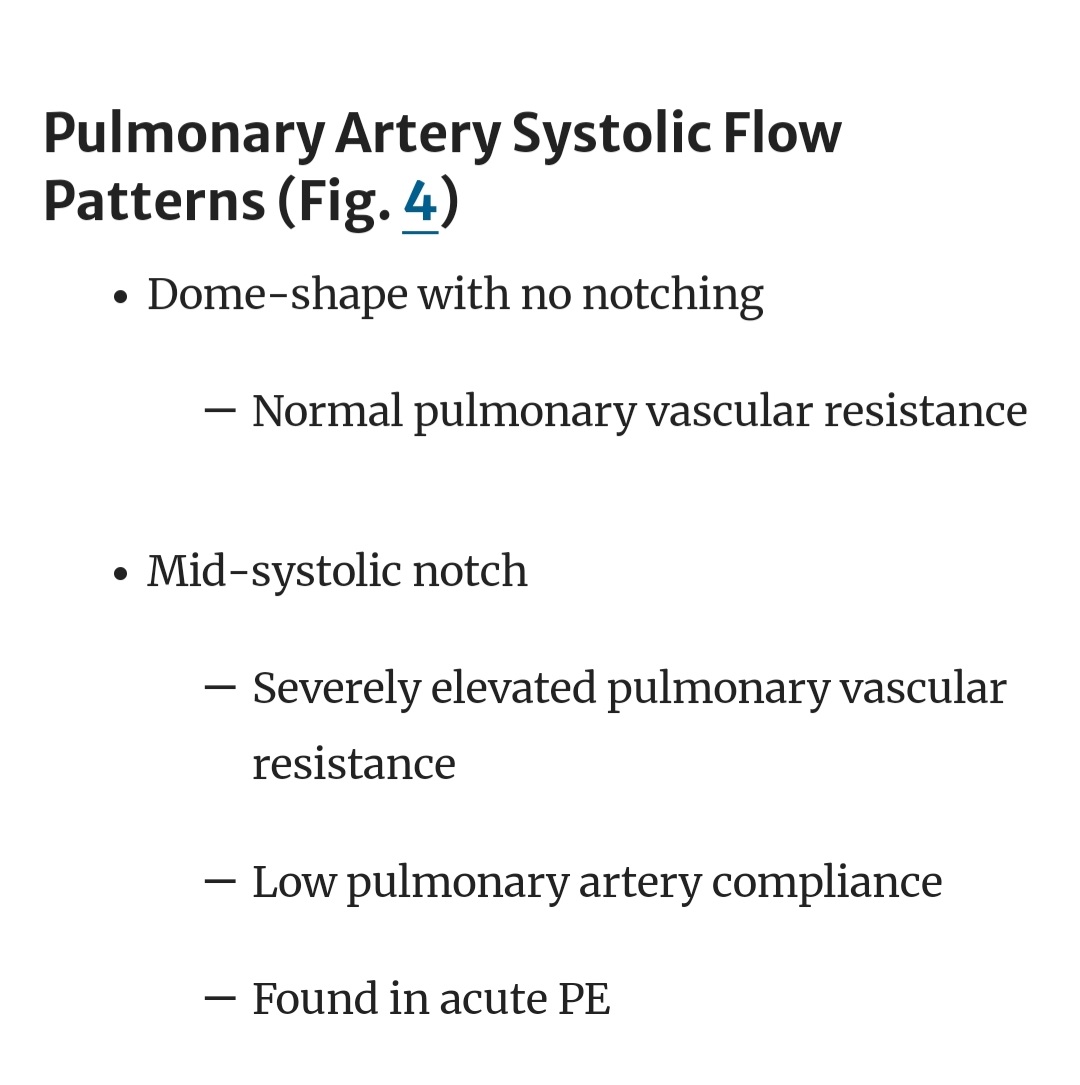
Estimation of pulmonary artery pressure using pulmonary artery acceleration time and Mid systolic Notch significance in the Waveform!
What's the mechanism behind Mid systolic notch in the Waveform?🤔
link.springer.com/chapter/10.100…
researchgate.net/figure/Schemat…


English
Dr Pakyto retweetou
💊BP lowering in CKD
1️⃣Step-ACEi/ARB+CCB/thiazide diuretic
2️⃣Step-ACEi/ARB +CCB+ Thiazide diuretic
3️⃣Step-Add Beta blocker/Spironolactone/central acting agent
@NDTsocial @hjanders_hans
doi.org/10.1093/ndt/gf…

English
Dr Pakyto retweetou
HOCM treatment algorithm
1. B blockers/CCBs(NDHP)
2. Disopyramide
3. Mavacamten(myosin inhibitors)?
4. Alcohol septal ablation vs Coil embolisation
5. AV sequential pacing
6. Surgical myectomy
7. Mitraclip
Avoid Vasodilators and high dose diuretics
researchgate.net/figure/Possibl…

English
Dr Pakyto retweetou

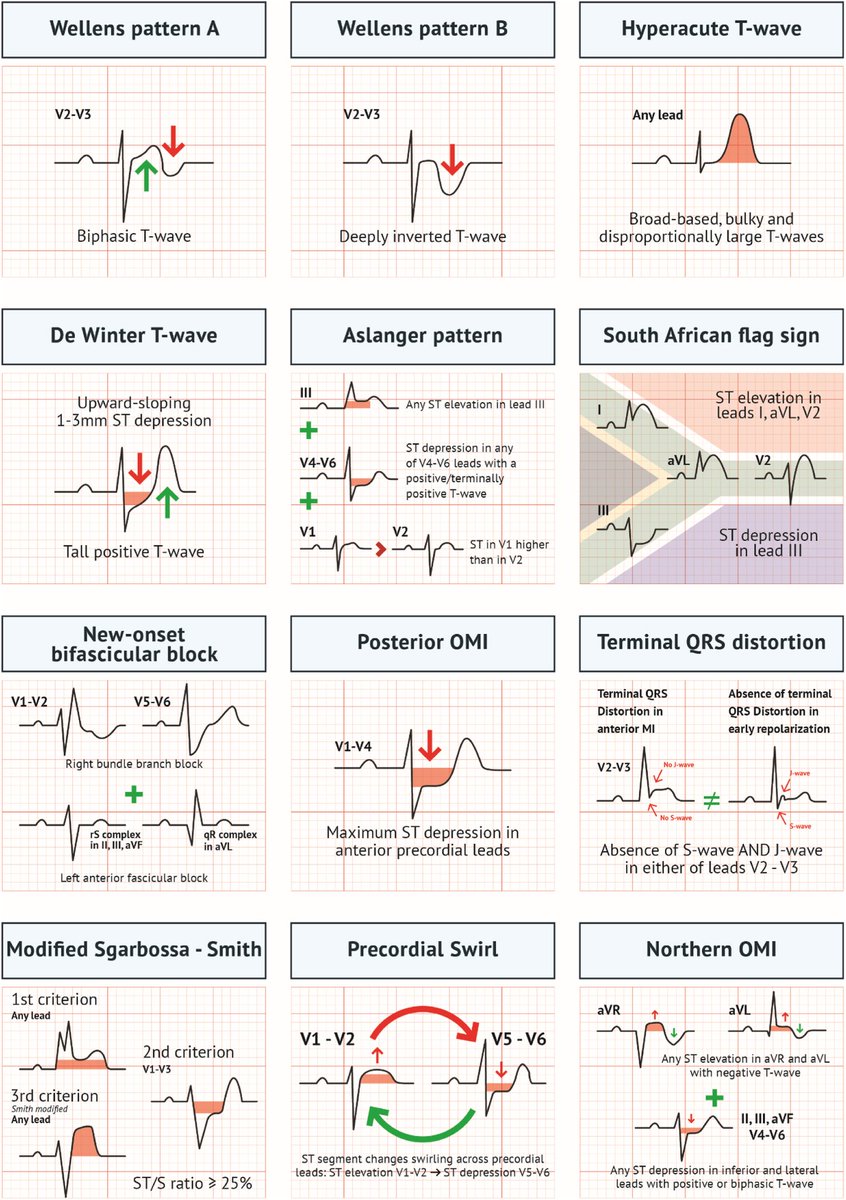
🔴ECG Patterns of Occlusion Myocardial Infarction:⤵️ #2025Review #OpenAccess @AnnalsofEM
🔹sciencedirect.com/science/articl…
#Cardiology #FOAMed #MedEd #medstudent #paramedic #Cardiology #CardioEd #medtwitter #meded #CardioTwitter #cardiotwiteros #MedX #cardiovascular

Dansk
Dr Pakyto retweetou

New England Journal of Medicine (NEJM) 2024: Trastorno por abuso de alcohol
DOI:10.1056/NEJMra2306511
#MedEd #MedTwitter #MedX

Dr Pakyto retweetou
Wellens syndrome >>>stuttering pattern of intermittent Reperfusion & Re-occlusion
Anterior STEMI >spontaneous clot lysis (Wellens with reperfusion T wave from biphasic to deep inverted T wave)> reocclusion again with Pseudo normalization of T wave >hyperacute T wave> STEMI


English
Dr Pakyto retweetou
Dr Pakyto retweetou

#Diabetes 🟠ACTUALIZACIÓN del 💊💉🏃♀️🥦Algoritmo de tratamiento de Diabetes Mellitus tipo 2 por el @SemergenGTDM
Descárgalo aquí: s.mtrbio.com/vhydovtzgb
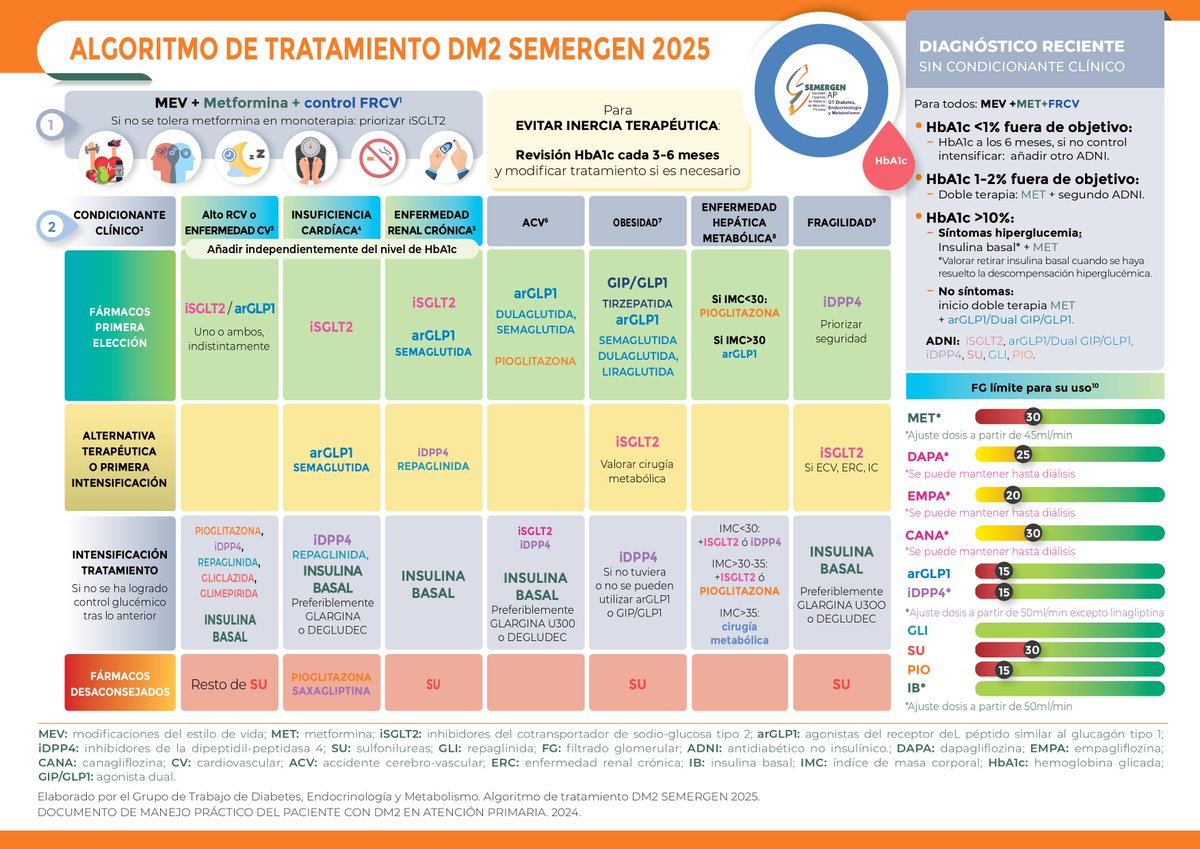
Español
Dr Pakyto retweetou

🌟 Introducing the Behçet’s Syndrome Overall Damage Index (BODI)!
🔍 A groundbreaking tool with 34 items across 9 organ systems designed to evaluate overall damage in patients.
📈 Demonstrated strong reliability (Cohen’s K = 0.73, ICC = 0.78) and sensitivity to changes over 5 years, making it essential in enhancing clinical outcomes.
🤝 Developed through collaboration with experts and patient input, it shows high feasibility in clinical settings with 94.1% acceptance among practitioners.
🔗 Explore more here: [10.1136/rmdopen-2020-001192](doi.org/10.1136/rmdope…)
#BehcetsSyndrome #BODI #ChronicIllness #HealthOutcomes #ClinicalResearch #DiseaseManagement #PatientCare #MedTwitter #RheumTwitter

English
Dr Pakyto retweetou

Obstrucción Intestinal - Signos de Indicación Quirúrgica Urgente 🔪
🔰📚Radiología 2023
doi.org/10.1016/j.rx.2…
Enlace a Artículo Completo 👇🏼✅🆓t.me/SoMELaguna


Español
Dr Pakyto retweetou

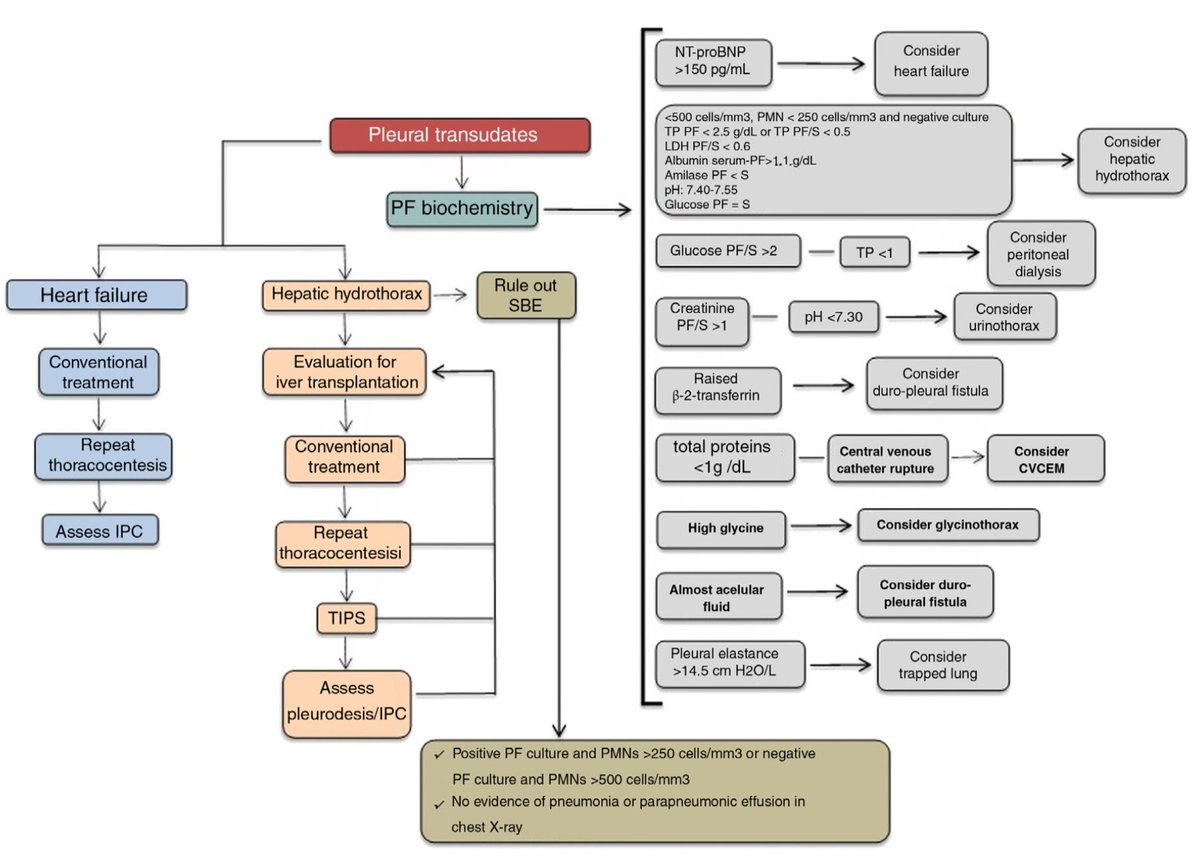
🩻𝗠𝗮𝗻𝗲𝗷𝗼 𝗱𝗲𝗹 𝗗𝗲𝗿𝗿𝗮𝗺𝗲 𝗣𝗹𝗲𝘂𝗿𝗮𝗹🫁
@Elsevier @ArchBronconeumo
👇🏼👇🏼👇🏼👇🏼👇🏼
🔗🔑🔓
buff.ly/42ktC1L
🧬𝗖𝗮𝘂𝘀𝗮𝘀 𝗺𝗮́𝘀 𝗰𝗼𝗺𝘂𝗻𝗲𝘀 𝗱𝗲𝗹 𝗗𝗣:
•Insuficiencia cardíaca (transudados).
•Neoplasias malignas (exudados malignos).
•Infecciones como neumonía y tuberculosis (exudados parapneumónicos o infecciosos).
•Otras causas: Pancreatitis, embolia pulmonar, hidrotórax hepático.
🩻𝗗𝗶𝗮𝗴𝗻𝗼́𝘀𝘁𝗶𝗰𝗼
•𝘾𝙧𝙞𝙩𝙚𝙧𝙞𝙤𝙨 𝙙𝙚 𝙇𝙞𝙜𝙝𝙩: Detectan exudados con 98% de sensibilidad, pero fallan en pacientes con diuréticos.
•Alternativas:
•Gradiente albúmina pleural/sérica >1.2 g/dL (mejor para diferenciar transudados con diuréticos).
•NT-proBNP >1500 pg/mL: Indica derrame asociado a insuficiencia cardíaca.
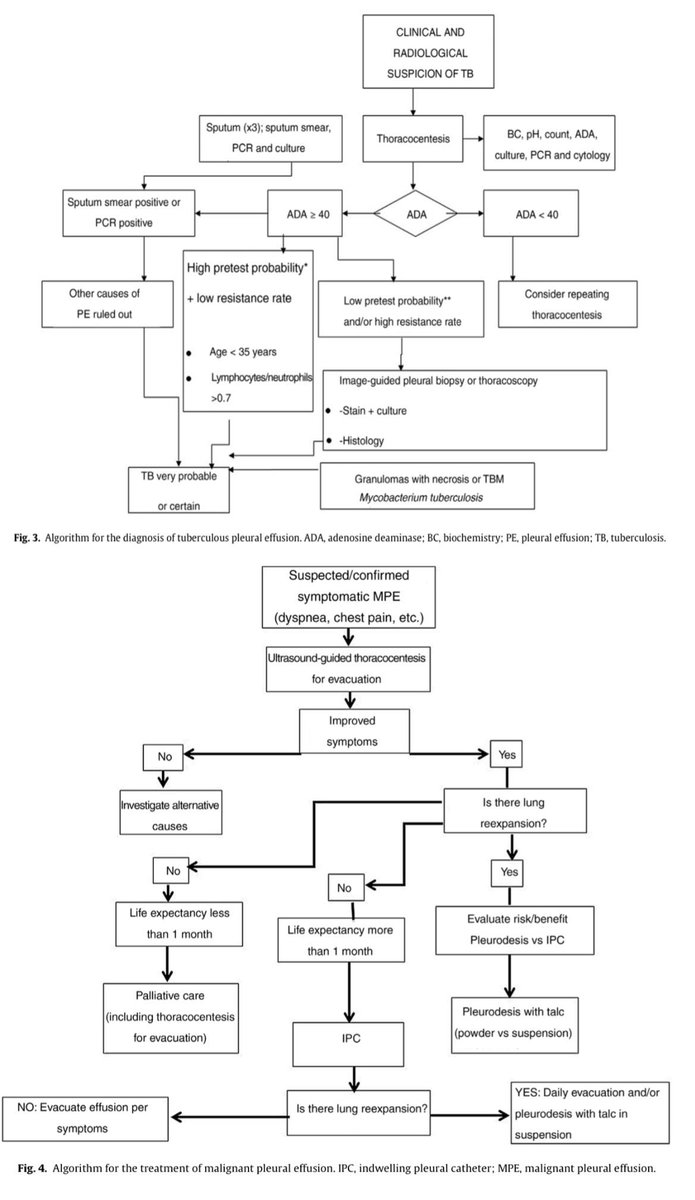
•𝘼𝘿𝘼: Sensibilidad del 92% y especificidad del 90% para tuberculosis pleural.
🧪𝗕𝗶𝗼𝗺𝗮𝗿𝗰𝗮𝗱𝗼𝗿𝗲𝘀 𝘆 𝘁𝗲́𝗰𝗻𝗶𝗰𝗮𝘀 𝗺𝗼𝗹𝗲𝗰𝘂𝗹𝗮𝗿𝗲𝘀:
•PCR para tuberculosis pleural: Mejora la sensibilidad en comparación con el cultivo convencional.
•INF-γ: Altamente específico para tuberculosis pleural en áreas endémicas.
•Citología pleural: Rendimiento del 49-91% para derrames malignos; la toracoscopía mejora la precisión.
🛠️ 𝗧𝗿𝗮𝘁𝗮𝗺𝗶𝗲𝗻𝘁𝗼 𝗱𝗲𝗹 𝗱𝗲𝗿𝗿𝗮𝗺𝗲 𝗽𝗹𝗲𝘂𝗿𝗮𝗹 𝘀𝗲𝗴𝘂́𝗻 𝗲𝘁𝗶𝗼𝗹𝗼𝗴𝗶́𝗮:
1️⃣ 𝙏𝙧𝙖𝙣𝙨𝙪𝙙𝙖𝙙𝙤𝙨:
•Insuficiencia cardíaca: Tratamiento con diuréticos resuelve el 89% de los casos.
•Hidrotórax hepático: Pleurodesis o catéter pleural en casos refractarios, trasplante hepático como opción definitiva.
2️⃣ 𝙋𝙖𝙧𝙖𝙥𝙣𝙚𝙪𝙢𝙤́𝙣𝙞𝙘𝙤 𝙮 𝙚𝙢𝙥𝙞𝙚𝙢𝙖:
•No complicado: Responde a antibióticos.
•Complicado o empiema: Necesita drenaje si pH <7.20 o LDH >1000 U/L.
•Terapias avanzadas:
•Antibióticos empíricos (piperacilina-tazobactam o carbapenémicos).
•Fibrinolíticos intrapleurales (ej. alteplasa) en derrames tabicados.
3️⃣ 𝘿𝙚𝙧𝙧𝙖𝙢𝙚 𝙥𝙡𝙚𝙪𝙧𝙖𝙡 𝙢𝙖𝙡𝙞𝙜𝙣𝙤 (𝘿𝙋𝙈):
•Pleurodesis con talco si el pulmón no está atrapado.
•Catéter pleural tunelizado (IPC) para manejo ambulatorio, especialmente en casos de pulmón atrapado.
🩻 𝗜𝗻𝗻𝗼𝘃𝗮𝗰𝗶𝗼𝗻𝗲𝘀 𝗲𝗻 𝗱𝗶𝗮𝗴𝗻𝗼́𝘀𝘁𝗶𝗰𝗼 𝘆 𝘁𝗿𝗮𝘁𝗮𝗺𝗶𝗲𝗻𝘁𝗼:
•Técnicas moleculares (PCR e INF-γ) mejoran la identificación de infecciones como tuberculosis pleural.
•Biopsias pleurales guiadas por toracoscopía son el estándar de oro en derrames malignos.
•Uso temprano de fibrinolíticos en empiemas complejos reduce la necesidad de cirugía.
📝 Resumen ampliado en el blog #ClubCrit
#icu #criticalcare #EducaciónMédica #DerramePleural #Diagnóstico #Tratamiento #uci #intensivecare #criticalcare #MedTwitter #FOAMed #FOAMcc #MedED #MedX #ICU #MedEd #MedXCommunity #edtech #education #LecturaRecomendada #EducaciónMédica #Medicina #medicaleducation #medicalstudent #internalmedicine #medicalpractice #MedX #CuidadoCrítico #MedicinaInterna #MedicalEducation #ClinicalCases #DoctorsOfTwitter #MedicalStudents #TecnologíaMédica


Español
Dr Pakyto retweetou
Such an excellent review of ECG findings in occlusion MI in @AnnalsofEM
A lot of value in reading and collaborating with our colleagues in other departments. Recommend reading!
sciencedirect.com/science/articl…

English
Dr Pakyto retweetou

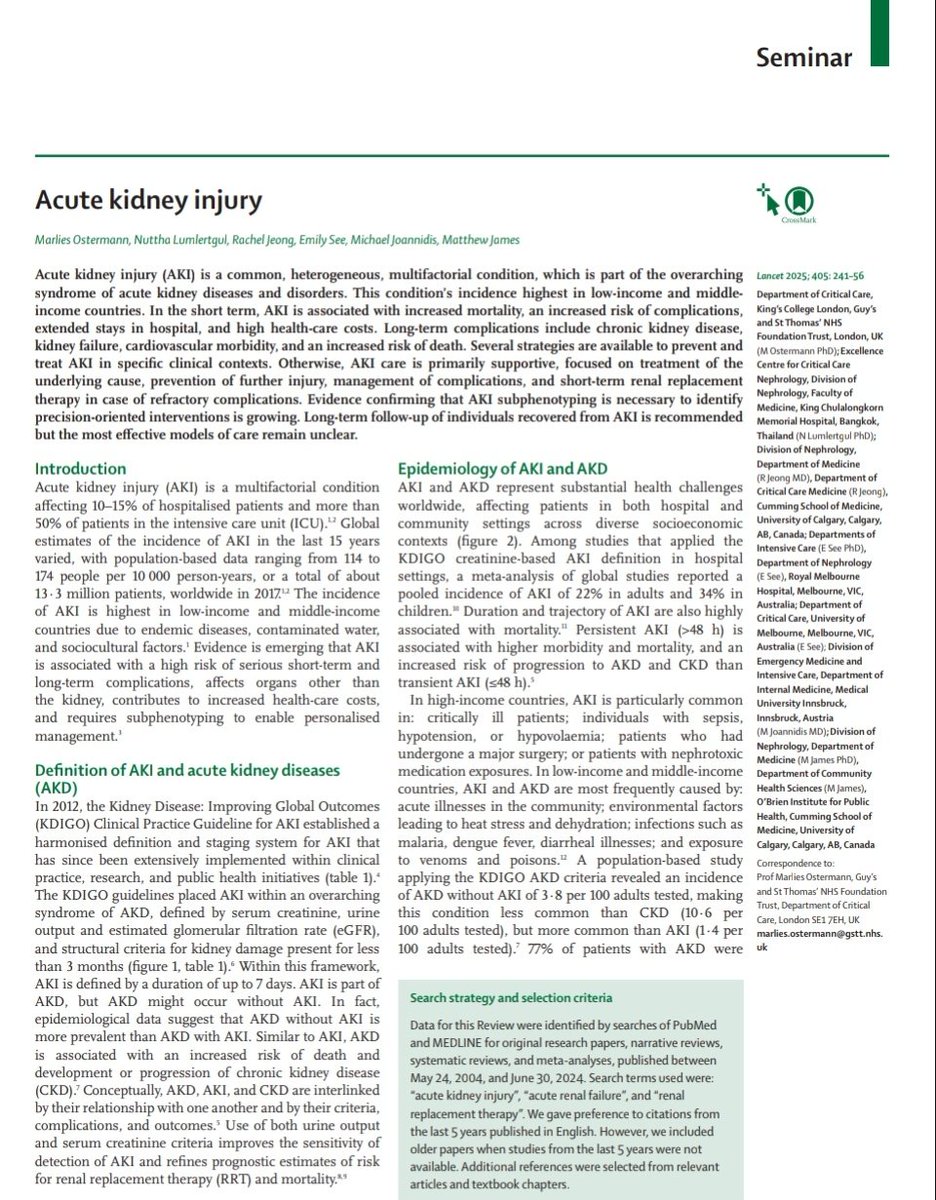
💎Lesión Renal Aguda 🫘
📖Definición
📊Epidemiología
🧬Fisiopatología
🩺Diagnóstico
💉Manejo
Pronóstico
🔰📚Lancet 2025
doi.org/10.1016/S0140-…
Enlace a Artículo Completo 👇🏼✅🆓t.me/SoMELaguna
Español
Dr Pakyto retweetou
🔴Beta-blocker and calcium-channel blocker toxicity: current evidence on evaluation and management⤵️ #2023Review
🔹academic.oup.com/ehjacc/article…
🔹pdf acrobat.adobe.com/link/review?ur…
#Cardiology #FOAMed #MedEd #medstudent #paramedic #Cardiology #CardioEd #medtwitter #meded




English
Dr Pakyto retweetou

💧 Understanding Fluid Accumulation Syndrome in Sepsis and Septic Shock 💧
🚨 Fluid Accumulation is a condition characterized by fluid overload leading to organ dysfunction—and provides insights into its pathophysiology, relevance, and management
linkedin.com/posts/manu-mal…

English
Dr Pakyto retweetou

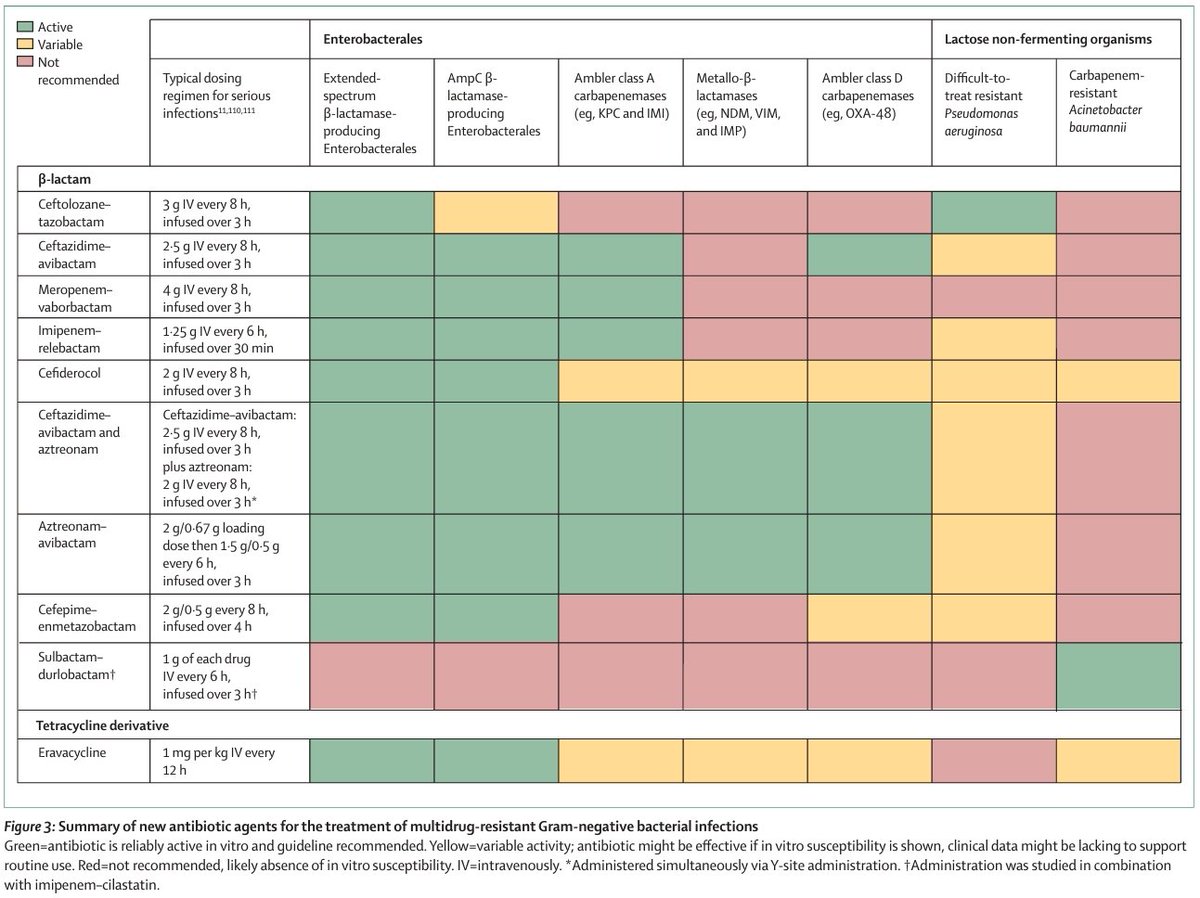
Summary of new antibiotic agents for the treatment of MDR Gram negative bacterial infections
doi.org/10.1016/S0140-…
English
Dr Pakyto retweetou

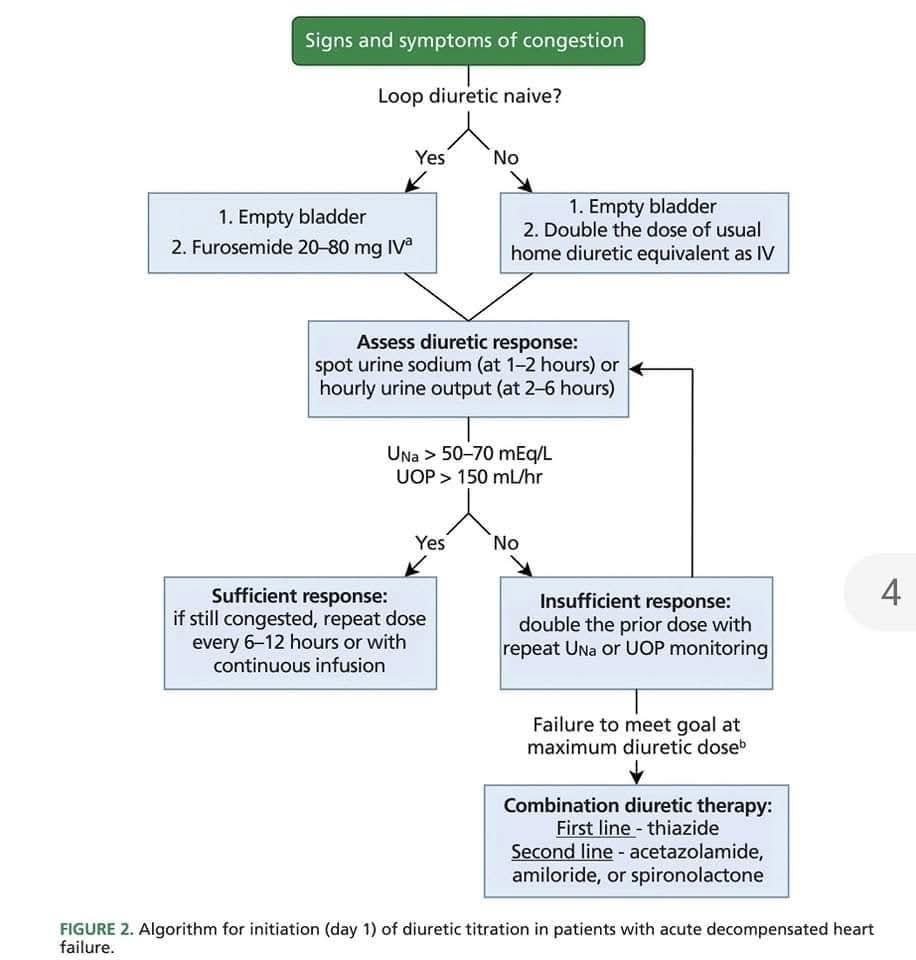
🧐¿Cómo maximizamos la diuresis💧 en la insuficiencia cardíaca aguda🫀 descompensada?🕤👩🏽⚕️👨🏼⚕️
✔️Se debe optimizar el diurético en función del NA y la diuresis💧
💊 Existe un umbral mínimo en la concentración tubular del diurético necesario para obtener respuesta, y un umbral 👇🏽

Español
Dr Pakyto retweetou

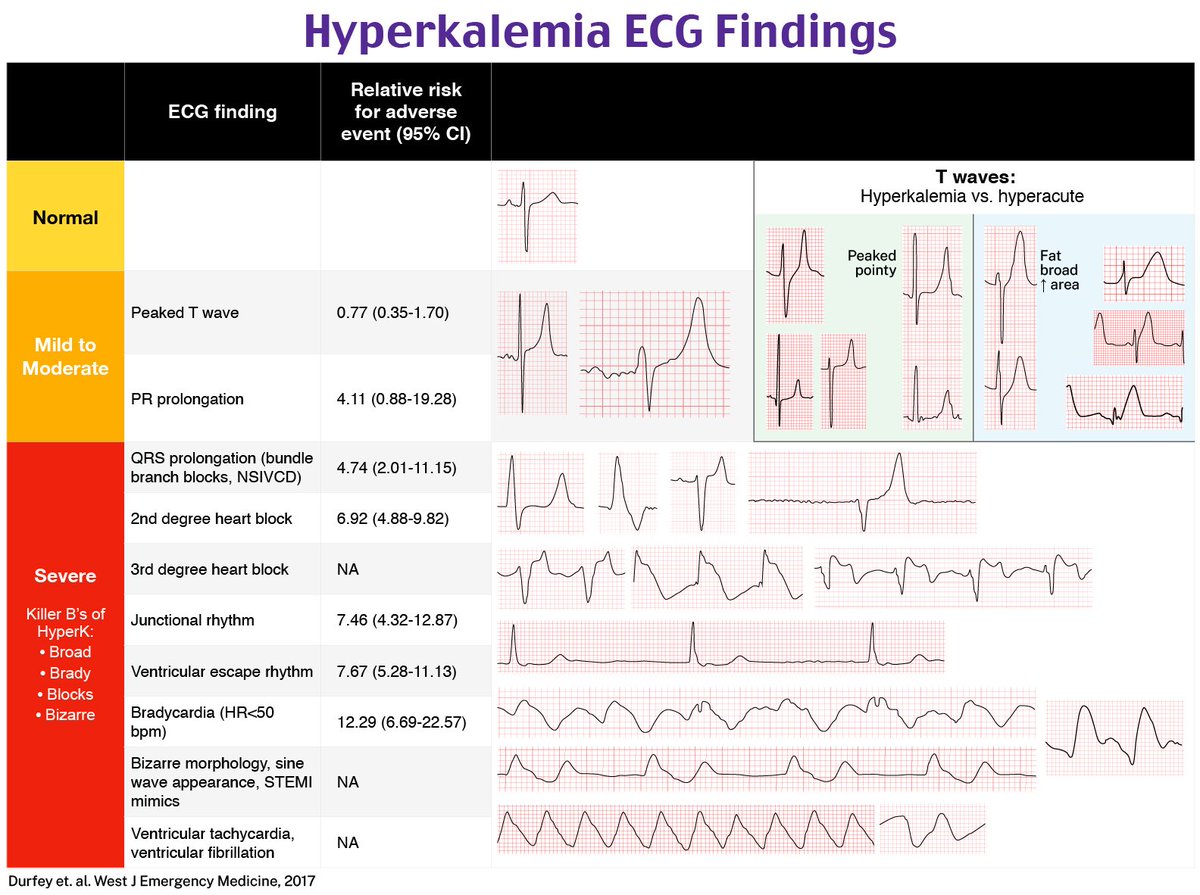
Hyperkalemia ECG Findings with Relative Risk (RR)
1️⃣ Normal: No changes (RR: N/A).
2️⃣ Mild to Moderate:
•Peaked T waves (RR: 0.77).
•PR prolongation (RR: 4.11).
3️⃣ Severe:
•QRS prolongation (RR: 4.74).
•2nd-degree block (RR: 6.92).
•3rd-degree block (RR: N/A).
•Junctional rhythm (RR: 7.46).
•Ventricular escape rhythm (RR: 7.67).
•Bradycardia (<50 bpm) (RR: 12.29).
•Bizarre morphology: Sine wave, STEMI mimic, V-tach, V-fib (RR: N/A).
T Waves
•Hyperkalemia: Peaked and pointy.
•Hyperacute: Fat and broad.
English
Dr Pakyto retweetou
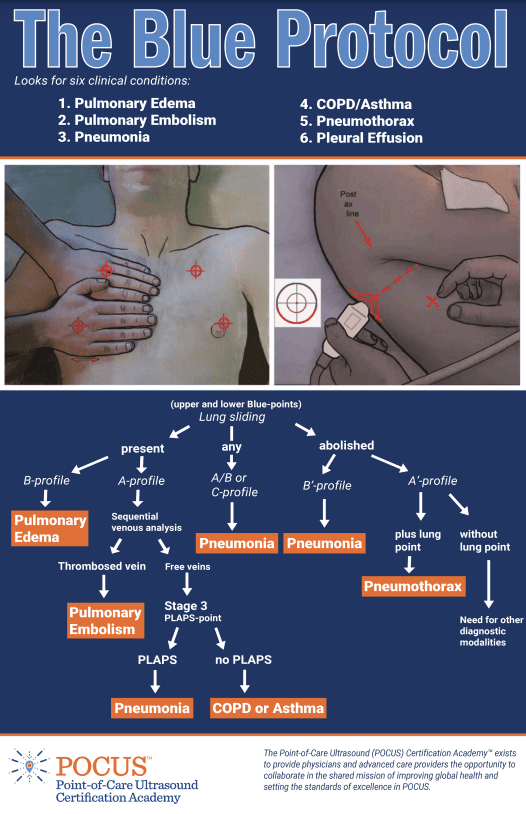
🔴Bedside Lung Ultrasound in Emergency (BLUE) Protocol⤵️ #openaccess
🔹The Bedside Lung Ultrasound in Emergency (BLUE) Protocol can help to quickly distinguish different lung pathologies.
🔹Download this quick reference infographic 👉 hubs.li/Q02Z33VB0
English