Right! You’ve already proven something most of the industry thought wasn’t possible: remove the spread, expose the real price, and make pharmacy costs deterministic.
The rest of employer healthcare hasn’t caught up. It still runs on price variance and unmanaged routing. If pricing opacity can be eliminated in pharmacy, then routing-driven cost variance across care delivery can be eliminated as well.
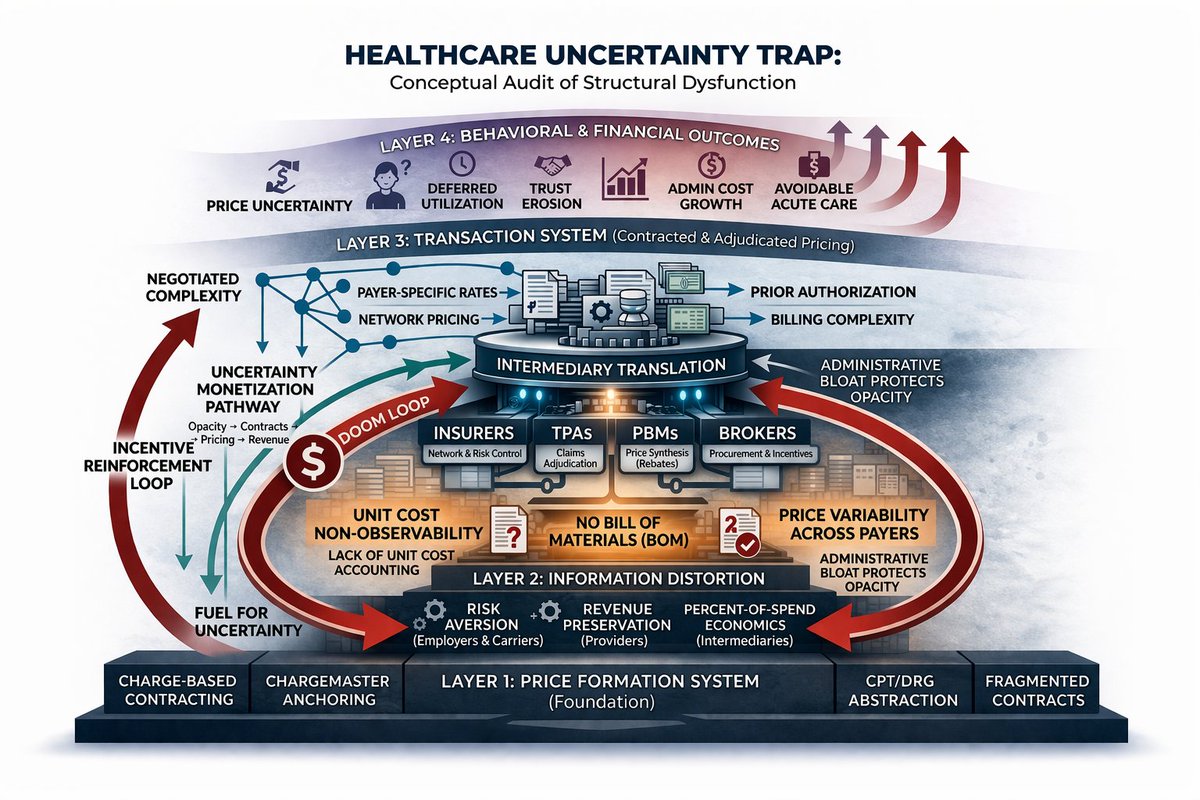
For the same clinical outcome, the system produces radically different costs:
A knee replacement can be $25,000 or $75,000
An MRI can be $500 or $3,000
An infusion can be $5,000 or $20,000
This isn’t a clinical problem. It’s a routing problem.
Today, no one controls where patients go before cost is incurred. As a result, the system monetizes that variance; hospitals capture it, intermediaries obscure it, and employers fund it.
The solution is to control the decision layer.
This is a routing and contracting platform that sits above the carrier and determines how care actually gets delivered. Every non-emergent entry point flows through a single front door. From there, a decision engine routes patients into pre-defined pathways with pre-priced bundles and enforced site-of-care. Instead of open-ended referrals, the system schedules the patient directly into the appropriate provider and setting.
The model only works if patients use it, so the incentives are immediate and tangible: zero out-of-pocket cost, end-to-end scheduling handled for them, and faster access than the default system. The right choice becomes the easiest one.
Operationally, this shifts healthcare from something that is negotiated after the fact to something that is routed in advance. Prices are locked before care occurs. Site-of-care arbitrage disappears. High-cost pathways, MSK, imaging, infusion, become standardized and predictable.
The business model mirrors the same principles that made Cost Plus compelling: fully transparent and aligned. A fixed platform fee on a per-employee basis, combined with a flat percentage of auditable savings. No spread, no hidden economics, just participation in the value created by eliminating unnecessary variance.
This doesn’t require replacing carriers or rebuilding the system from scratch. It simply places control where it has never existed, at the point where decisions are made. Whoever controls where the patient goes, what gets done, and what gets paid controls the economics.
I know you’ve assessed this thoroughly.
But what’s your take on if you start with a narrow, high-yield focus on MSK and imaging, areas where price dispersion is extreme, routing is controllable, and results can be demonstrated quickly.
The immediate objective being to run a pilot within one of your portfolio companies, applying this model end-to-end to prove a measurable 20–30% cost reduction within 18 months. To ensure clean execution and credible results, the pilot should target a population of roughly 5,000–10,000 covered lives, with the majority concentrated in one or two core metro areas.
That level of density provides enough repeatable event volume (surgeries, imaging, infusions) and sufficient provider optionality to enforce routing, lock pricing, and produce defensible savings.
The scope is intentionally constrained: focus on markets where alternative sites of care exist (ASCs, independent imaging) and where routing can be operationalized without friction. This ensures that savings are not theoretical, but observable and attributable.
A 5,000–10,000 life pilot costs roughly $2–6M annually, driven primarily by a $30–$50 PEPM platform fee plus incentives and setup. It targets $1–6M in first-year savings from MSK and imaging alone, with stronger ROI in year two as adoption and contracting scale. The goal isn’t short-term arbitrage, it’s proving that controlling routing reliably converts variance into repeatable savings.
Or tighter starting at $20–$30 PEPM and narrowing the scope further (imaging-only entry wedge).
English