Yvan Maque รีทวีตแล้ว

🌞 Malar Rash: Beyond Lupus
A malar rash is an erythematous rash over the cheeks and bridge of the nose, classically resembling a butterfly.
Not every malar rash is lupus
Here are a few differentials of malar rash👇👇
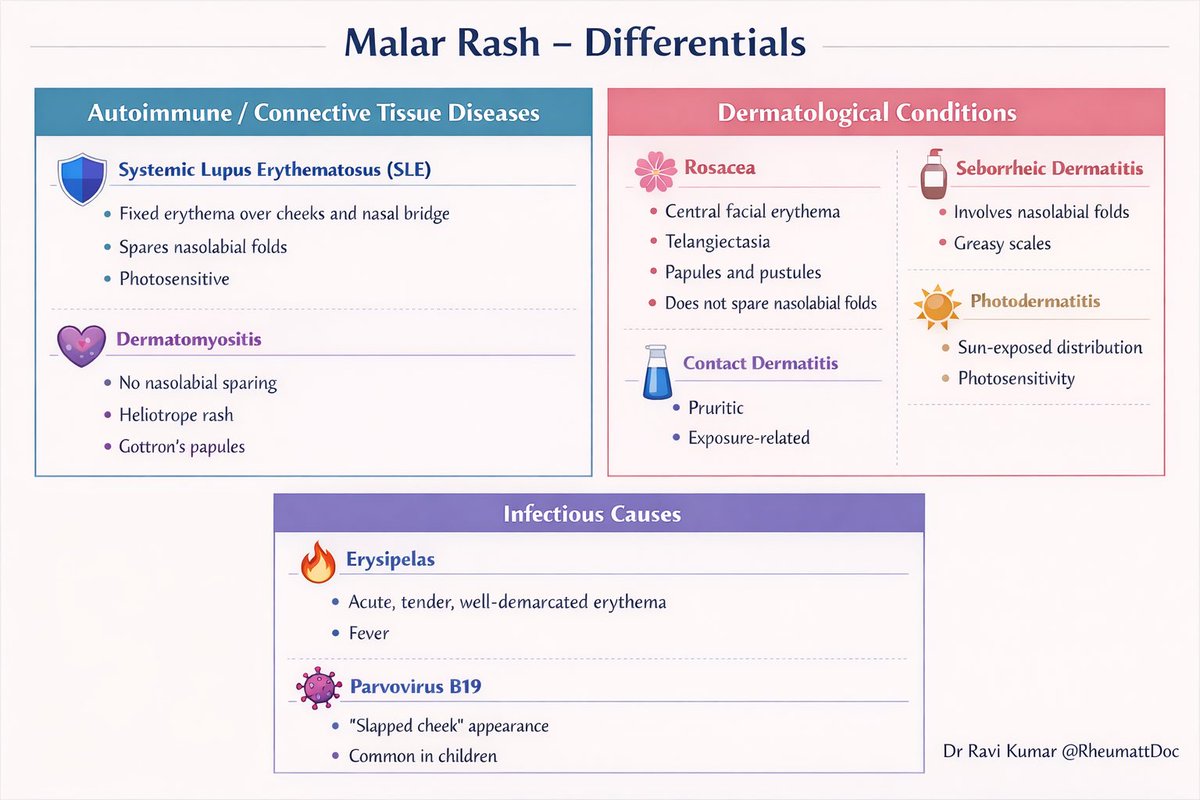
🧠 Rheumatological Conditions
🛡️ Systemic Lupus Erythematosus (SLE)
•Fixed erythema over cheeks and nasal bridge
•Spares nasolabial folds
•Photosensitive
💜 Dermatomyositis
•Does NOT spare nasolabial folds
•Heliotrope rash
•Gottron’s papules
•Proximal muscle weakness
🌿 Dermatological Conditions
🌸 Rosacea
•Central facial erythema
•Telangiectasia
•Papules and pustules
•Does not spare nasolabial folds
🧴 Seborrheic Dermatitis
•Prominent involvement of nasolabial folds
•Greasy yellow scales
☀️ Photodermatitis
•Sun-exposed distribution
•Clear photosensitivity history
🧪 Contact Dermatitis
•Pruritic eruption
•Exposure related
🦠 Infectious Causes
🔥 Erysipelas
•Acute onset
•Tender, well-demarcated erythema
•Fever and systemic symptoms
🧫 Parvovirus B19
•“Slapped cheek” appearance
•More common in children
•Often associated with viral prodrome
#RheumattDoc #MedTwitter #RheumTwitter #Medicine #rheumatology @DrAkhilX @IhabFathiSulima @CelestinoGutirr @DurgaPrasannaM1
English