
AT
845 posts


AT nag-retweet

$ERAS $ANL
$ERAS were idiots how they played this game. Should not have been dragged into $RVMD scenario and be reactive. Should have waited and released mature data.
But to say that Big Pharma will just give up a $10-15B market and leave it all to $RVMD is ridicules.
Saying "RVMD will get approved first and take the whole market" is plain stupid. Never happened before.
There are many strategies Big Pharma can play with: first line, combinations.....
There is no way, because there is just no way. that this market will be left to $RVMD to play in alone.
And there are only two ways you can play this theme in public markets : $ANL or $ERAS.
All in all I think $ANL is the winner from the late $RVMD - $ERAS debacle.
Ohad Hammer@ohadhammer
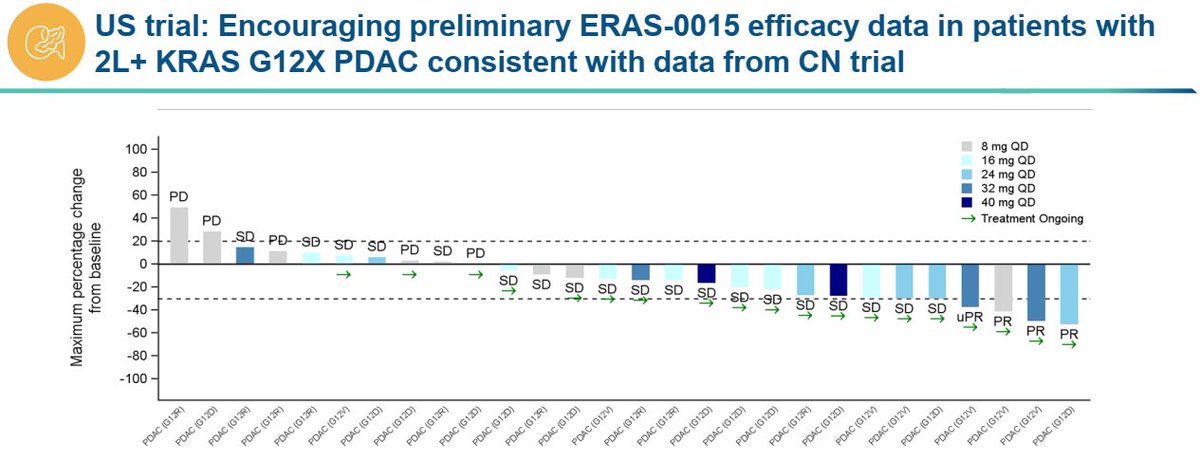
Putting criticism about timing and data presentation aside, $ERAS' ERAS-0015 seems very similar to $RVMD's daraxonrasib imo. ERAS-0015 is more potent which explains the lower exposure required for efficacy (and associated with on target toxicity of course). It might have a slight advantage on GI side effects (to be seen) but other than that it is likely to have a similar therapeutic index. If we compare just the PDAC data sets, $ERAS reported 4 PRs in 21 patients (~19% ORR) in the US at relevant doses which is lower than dara's 35% ORR but that gap will likely close with more follow up as $ERAS has multiple near PRs at the first scan than can convert in the future (They need 3 such conversions to reach 33% ORR). The limited follow up probably has a confounding effect on safety as well (longer treatment typically leads to more side effects) which should take $ERAS to a similar dose interruption/reduction rate in the future. Gr5 pneumonitis case requires attention but it could be an isolated case. Is $ERAS cheap at $3B? Not sure but for pharmas who cannot afford or simply won't get $RVMD this is the closest fast follower program that could be P3 ready later this year. *no position in stocks mentioned *
English
100% agree. $ERAS got a beating that may have been well deserved given the the bloated valuation and hastened data report, but remains, along with $ANL, the only playable RAS names. $ANL much cheaper and with less of a patent overhang should pickup ahead of data.
Ohad Hammer@ohadhammer
Putting criticism about timing and data presentation aside, $ERAS' ERAS-0015 seems very similar to $RVMD's daraxonrasib imo. ERAS-0015 is more potent which explains the lower exposure required for efficacy (and associated with on target toxicity of course). It might have a slight advantage on GI side effects (to be seen) but other than that it is likely to have a similar therapeutic index. If we compare just the PDAC data sets, $ERAS reported 4 PRs in 21 patients (~19% ORR) in the US at relevant doses which is lower than dara's 35% ORR but that gap will likely close with more follow up as $ERAS has multiple near PRs at the first scan than can convert in the future (They need 3 such conversions to reach 33% ORR). The limited follow up probably has a confounding effect on safety as well (longer treatment typically leads to more side effects) which should take $ERAS to a similar dose interruption/reduction rate in the future. Gr5 pneumonitis case requires attention but it could be an isolated case. Is $ERAS cheap at $3B? Not sure but for pharmas who cannot afford or simply won't get $RVMD this is the closest fast follower program that could be P3 ready later this year. *no position in stocks mentioned *
English
AT nag-retweet

Putting criticism about timing and data presentation aside, $ERAS' ERAS-0015 seems very similar to $RVMD's daraxonrasib imo.
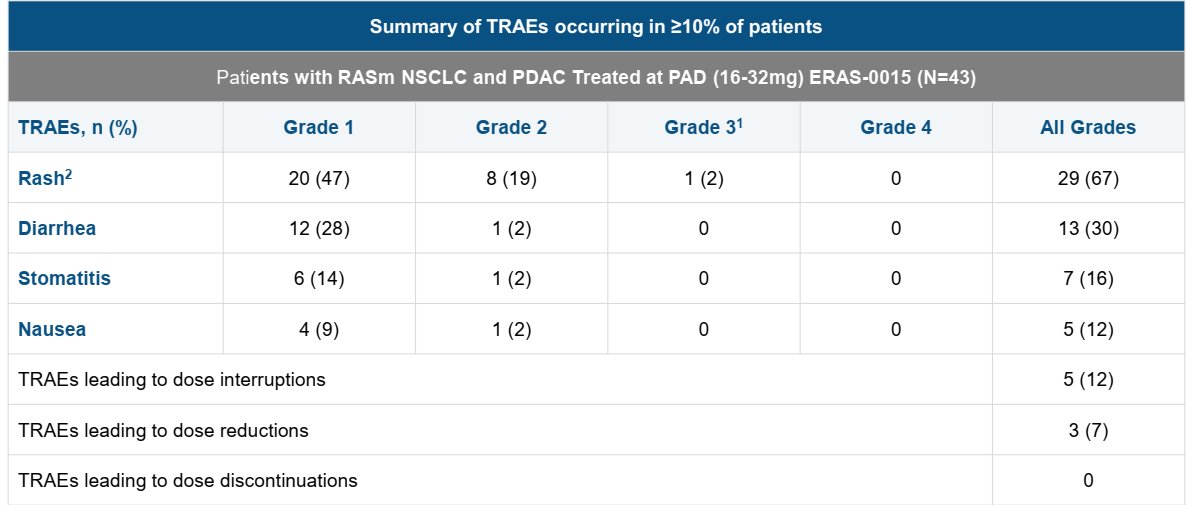
ERAS-0015 is more potent which explains the lower exposure required for efficacy (and associated with on target toxicity of course). It might have a slight advantage on GI side effects (to be seen) but other than that it is likely to have a similar therapeutic index.
If we compare just the PDAC data sets, $ERAS reported 4 PRs in 21 patients (~19% ORR) in the US at relevant doses which is lower than dara's 35% ORR but that gap will likely close with more follow up as $ERAS has multiple near PRs at the first scan than can convert in the future (They need 3 such conversions to reach 33% ORR).
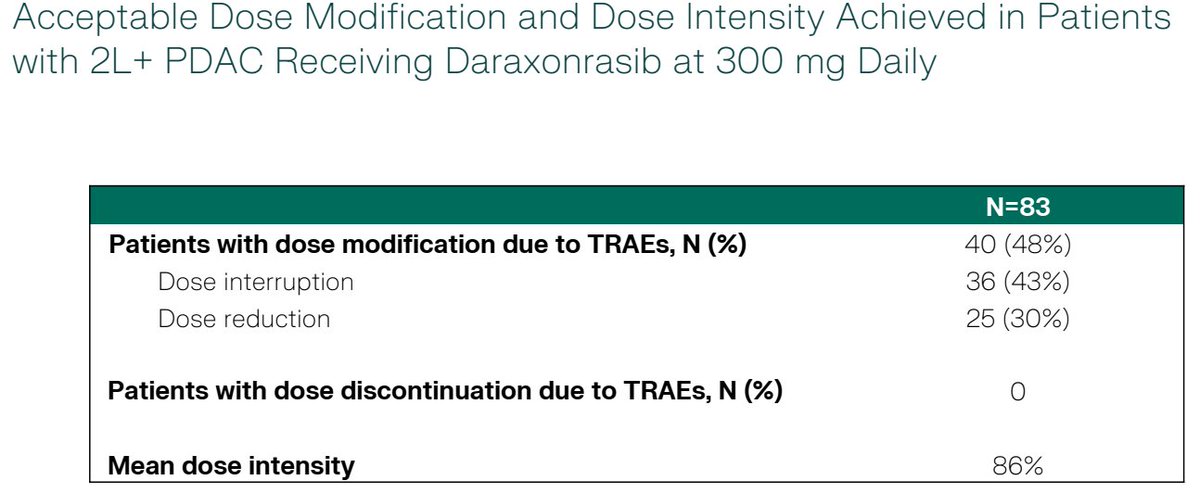
The limited follow up probably has a confounding effect on safety as well (longer treatment typically leads to more side effects) which should take $ERAS to a similar dose interruption/reduction rate in the future. Gr5 pneumonitis case requires attention but it could be an isolated case.
Is $ERAS cheap at $3B? Not sure but for pharmas who cannot afford or simply won't get $RVMD this is the closest fast follower program that could be P3 ready later this year.
*no position in stocks mentioned *

English
$ERAS re lawsuite, anyone who follows this space closely couldn't be surprised. I view it as an acknowledgement by $RVMD that ERAS is a threat, despite the lag. Re data, I think they have a good molecule on their hands. With RVMD @ $30B, what other way to play RAS? $ERAS $ANL
English
True, but most likely not a real signal given the context of the disease and history of the patient. Not a big deal IMHO. Overall tolerability profile is actually encouraging $ERAS
WC@Sanctuary_Bio
have to say really not a great look to not disclose a death in the PR and only mention it in slides. If there really is no correlation, what's the issue
English
So $ERAS got the letter from $RVMD on Friday and decided during the weekend to give a data update on Monday?
Adam Feuerstein ✡️@adamfeuerstein
$ERAS pan-Ras data update this afternoon after market close. also, $RVMD sent Erasca a letter claiming ERAS-0015 violates certain RevMed patents. sec.gov/Archives/edgar…
English
AT nag-retweet


$IDYA biggest takeaway from the call is mgmt noting early separation of OS curves with 10m of follow up
Jacob Plieth@JacobPlieth
$IDYA PFS curves from Optimum-02
English
AT nag-retweet


AT nag-retweet

$IDYA
EV of $2B
Will dominate Uveal Melanoma for years. $1-2B in Us plus royalties Ex-US.
Massive pipeline.
English
AT nag-retweet

mPFS, HR, ORR as expected
5 CRs a nice suprise
NDA 2H 26, new SOC for hla-
$IDYA Balance sheet is strong. No competition, small # of docs - marketing cost shouldn't be exorbitant. Could book rev early '27 to fund rest of pipe.
media.ideayabio.com/2026-04-13-IDE…
English
$IDYA mUM market is theirs for the taking. Uptake will be fast.
financebully@financebully
$idya easy choice for patients, docs and payors. hr = 0.42💥💊 4x fewer g3+ traes.
English
AT nag-retweet

The world is truly upside down! The Washington Post has published a brilliant article, written by, get this, a professor! To give you some flavor, here are a few choice lines by @jmurtazashvili:
1) "We are living through the first alt-war: a conflict in which the war fought online and the war fought in reality have diverged so completely that they might as well be happening on different planets. It’s not that people lack information, it’s more that they are constructing an entirely different alternate reality — one that confirms what they already believe."
2) "What worries me more than the fake videos are the people who cannot fathom that this war is going well for the United States, for Israel and maybe even for the long-suffering people of Iran. The strategic picture is more favorable than the online narrative suggests."
3) "Two weeks into the war, I watch otherwise reasonable analysts sprint to catastrophe. Former officials, thinktank scholars, credentialed professionals who are supposed to know how to read a conflict. Within days they had written the obituary: quagmire, overreach, disaster."
4) "The liberal internationalist left and the isolationist right — two camps that have agreed on almost nothing for decades — have suddenly found themselves in lockstep, racing to declare the war a failure before it had barely begun. This is the new blob: not the old foreign-policy establishment that the term originally described but a new amalgamation that has arrived at the same conclusion from opposite directions. Together they are the most powerful engine of the alt-war."
The truth. In the mainstream media. By a professor. And written well. Four things I thought I'd never see again in my lifetime.

English
AT nag-retweet
$AVTX
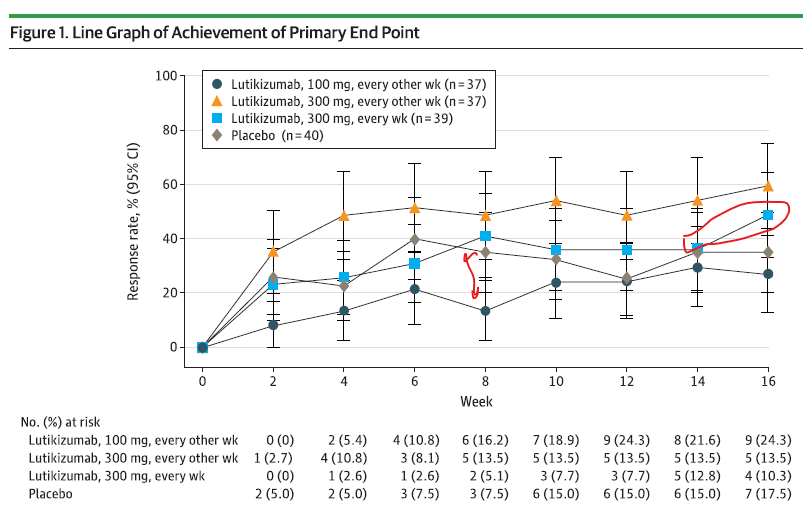
Lutikizumab HS data is out and in my view it does not look great in my view.
This is supposed to be the "strongest bullish" argument for $AVTX.
HiSCR50- the high dose looks exactly as placebo and had a strange bump between week 14 and 16.
The low dose looks worse than Placebo.
English
AT nag-retweet

Efficacy down a bit but still very decent, prophylaxis working well
Sometimes thesis just stares you right in the face $ctmx
WC@Sanctuary_Bio
@anthonystaj I'm not overly worried about this. Prophylaxis should help. We've seen in trials as recent as HERIZON-GEA-01 that you can bring gr3 diarrhea way down. That one still had 24.5% gr3 diarrhea with a 11.9% d/c rate after prophy. Not atrocious all things considered.
English