
Arsh
409 posts


@CannulaTech Hi, thank you for your messages! The "infusulator" will work separately from the main app functions. To access the "infusulator", you can use the "research mode", which is available on the front screen. I shall introduce more about the feature soon
English
"Infusulator", first created by Dr. Matthew Hart, to be incorporated into SimTIVA. It allows easy entry of a time series of CE (or CP) targets to generate TCI simulations. The conversion from CET/CPT to dosage (volume infused, or the total dose) over time is made simple. An export module is also provided.
English
Arsh nag-retweet

In France:
• incidence of hypersensitivity reactions related to sugammadex appears to be low
• observed clinical presentations & severity are broadly comparable, with cardiovascular symptoms predominating +/- cutaneous & respiratory manifestations
#anaesthesia #allergy #MedTwitter
doi.org/10.1111/anae.7…
English
Faracial to think that very capable foundation and post foundation docs are left scrambling for training posts, at time when we need more specialists.
I think this issue re: employment/progression needed to (and needs to) be front and centre in public domain.
Most are oblivious
English
@TheSnoozeDoctor Somethings got to break tbh. Question is when and what.
I’ve seen this go parabolic in the past 3-5 years.
English
@JAShuttleworth @rachelgemma90 Sorry to hear that.
Great you’ve made the cut, pretty sure it can only get better.
English

@rachelgemma90 Same for me - appointable but not offered the DSAA job, try again next year
English

No PHEM training number for me this year. Ranked as appointable but not highly enough to get either of the West Mids posts.
English
@simtiva_app Would love to play around with these.
The app massively helps plan for RSIs that I plan to run on volatile but would love to have information from pk/pd modelling to help plan peri-induction period.
Although i hope the current non-infusulator interface will stay as well.
English
@doctimcook I think C&L scores are a bit like ASA gradings. Based on vibes.
English

The original Cormack and Lehane paper
-widely cited
-but how well do you know it?
Tim Cook@doctimcook
Most means more than half. So for POGO it’s anything >50% It’s a common misconception that grade 1 means ‘full view of the cords’ The C&L grading is more often incorrectly quoted then correctly quoted in papers The original Cormack and Lehane paper had multiple issues. pubmed.ncbi.nlm.nih.gov/6507827/ One is that thee are no data and wildly inaccurate (overoptimistic) estimates of how infrequent Grade 3 & 4 views are. Estimate grade 3 1:2000 and grade 4 <1:100,000. These are fanciful: grade 3 is 5.8% The second is that the images of grades don’t match the text description. This includes that in the Grade 3 image posterior laryngeal structures are clearly visible The third and final problem with the C&L paper is that the grades don’t correlate with increasing difficulty with intubation. Difficulty increases -mid grade 2 (need a bougie) -in grade 3 if you can’t lift the epiglottis (need to do something fancy) This is resolved by the practical grading published in 2000 by some whippersnapper upstart …-publications.onlinelibrary.wiley.com/doi/full/10.10… In summary The paper has no data The estimates of incidence are wildly inaccurate The scale is imprecisely described The scale is very poorly remembered and quoted The scale is of very limited practical value Apart from that it’s great… @Anaes_Journal @dasairway
English
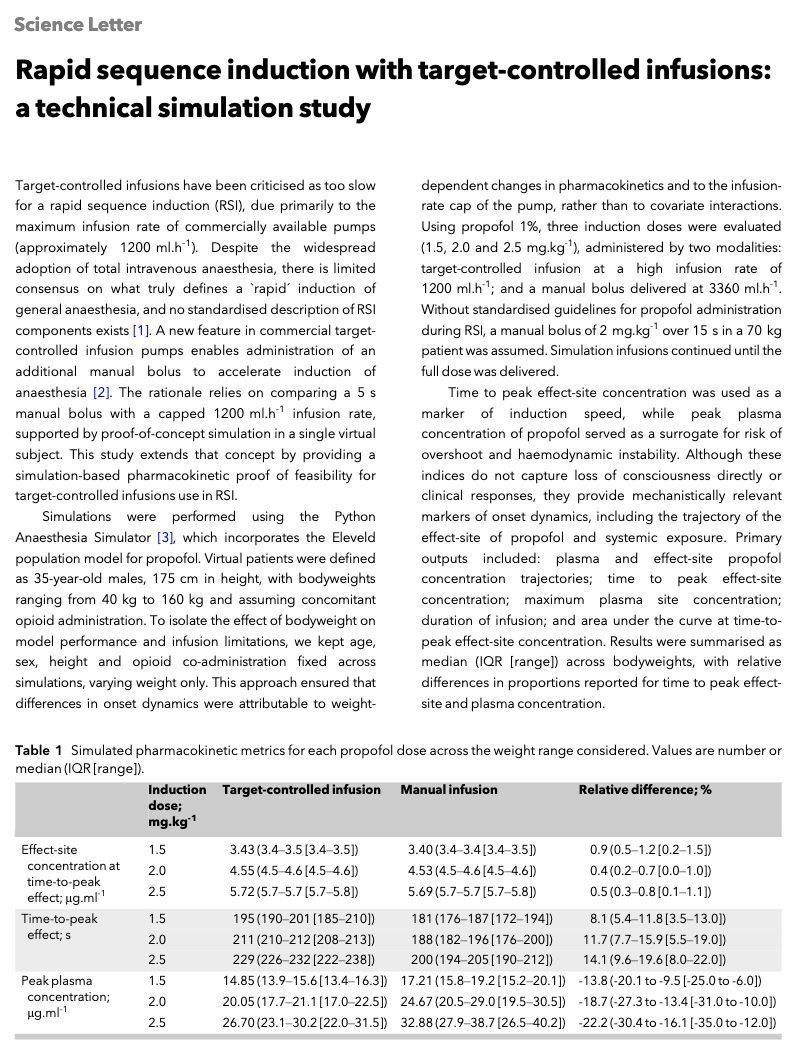
@Anaes_Journal I find this rather interesting because usual bolus speeds are closer to 7200ml/hr or 2ml/sec
A 2.5mg/kg bolus given via 7200 vs 1200 ml/hr would lead to significantly different time to peak conc and peak effect site, and plasma conc.
Manual rates in this err conservative imo
English
Rapid sequence induction with target-controlled infusions: a technical simulation study
#anaesthesia #MedTwitter
doi.org/10.1111/anae.7…
English
Conclusion?
“More research is needed in this area”
Although if I take my trainee/clinician hat off and put a managerial, cost efficiency hat on - it’s not hard to extrapolate that non-physician providers are largely without significant adverse effects.
British Journal of Anaesthesia@BJAJournals
This #RCoA commissioned mixed-methods #systematicreview looks at the role of and working models of non-physician providers of #anaesthesia in high-income countries - what evidence exists in the literature? bjanaesthesia.org.uk/article/S0007-…
English
@Resuspiece @AbbieTBee Gave me a panic the other week.
Dental extraction list on little kiddies
LMA got yanked, kid went from sats 97% to 67% before I could welp D:
They are cute though. Cute and scary.
English

@AbbieTBee Do some Paeds lists!! Doesn’t even feel like a day at work
English


NHS doctor here, Rupert. If you'd checked your facts before this racist dogwhistle, you'd know that every NHS doctor can speak English - as proven by their IELTS proficiency (look it up... or are you just a populist hatemonger for whom facts don't matter?). Kindness may not solve everything, but my God the hate you spew is builds nothing, improves nothing, and only stokes division.
Rupert Lowe MP@RupertLowe10
A comment which sums up the mad delusion of many on the left. ‘Kindness’ can overcome migrant language issues in the NHS, I’m told. Good luck with that. I’ll go with the doctor who can actually speak English, thanks.
English
Arsh nag-retweet

Guay et al. review frontal EEG signatures organized into an active management framework that integrates traditional drug signatures with the pathophysiology of critical illness to guide active management of critically ill patients. Learn more: ow.ly/r21150XqbMt
English
@Resuspiece @ACEPNation new guidance looks solid in this regard. Much more trust and reliance on flush rate nasal cannulae, NRBM and bipap in higher risk cases. Thoughts?
English
We are going to need to develop strategies in peroxygenation
Hugh Hemmings@HughHemmings
Release of 2025 DAS guidelines! Plan, Peroxygenate, Communicate! Available OA @BJAJournals #WAMM2025
English
@jinnieshinnie It’s all A-E exams, which you can teaching to any lay person.
Not a single student has heard of MacLeods or a textbook akin to that.
We have restructured med ed in the UK to train workers to work on conveyer belt of healthcare.
English
@jinnieshinnie Although I do stand with and echo your opinion, having taught medical students in a formal role as recently as two years ago, none of them reading primary texts or referring to basics.
It’s all online question banks for exams and protocols for clinical practice.
English

Louder for the people in the back (and those responsible for doctor substitution and medical training degradation in the UK)!!
A solid foundation better equips you for solving problems. A protocol will cover a lot but you need a doctor to know when it is insufficient.
Whitfield Lewis, MD 🇦🇬🇺🇸@whitfieldlewis6
A young doctor asked me, “Why keep reading basic science?” Well, where to start? You never want to reduce your practice to robotically following algorithms and protocols — though those checks and balances have their place in patient care. As a neurologist, I don’t see reading about neuroanatomy, localization in clinical neurology, neurochemistry, physiology, and biochemistry as “going back” to the basics. Basic science enhances your ability as a clinician, a surgeon, or a radiologist. For me, it helps make better sense of patients’ symptoms, exam findings, and imaging results. If you don’t know which lesions cause which symptoms, you can’t connect seemingly isolated findings or unusual presentations. Medicine isn’t just about memorizing patterns — it’s about understanding the underlying systems well enough to navigate the gray areas, interpret data correctly, and choose treatments with insight.
English