Naka-pin na Tweet

Last few days for early bird! Join us in Montreal next september! #HR26 Nothing quite like it... thinkingcriticalcare.com/2026/01/16/fou…
English
Philippe Rola
23K posts

@ThinkingCC
#zentensivist, EMCrit Teammate, Proud daddy and husband. BJJ🟪. ICU Santa Cabrini Hospital.

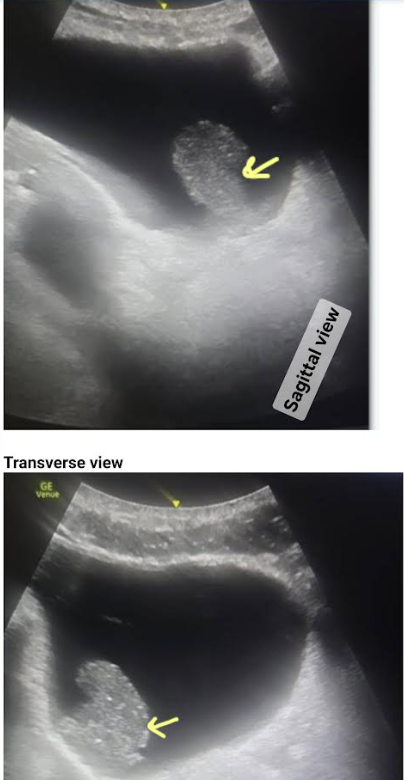
What is the most reasonable immediate next step?