Healthcare costs accumulate.
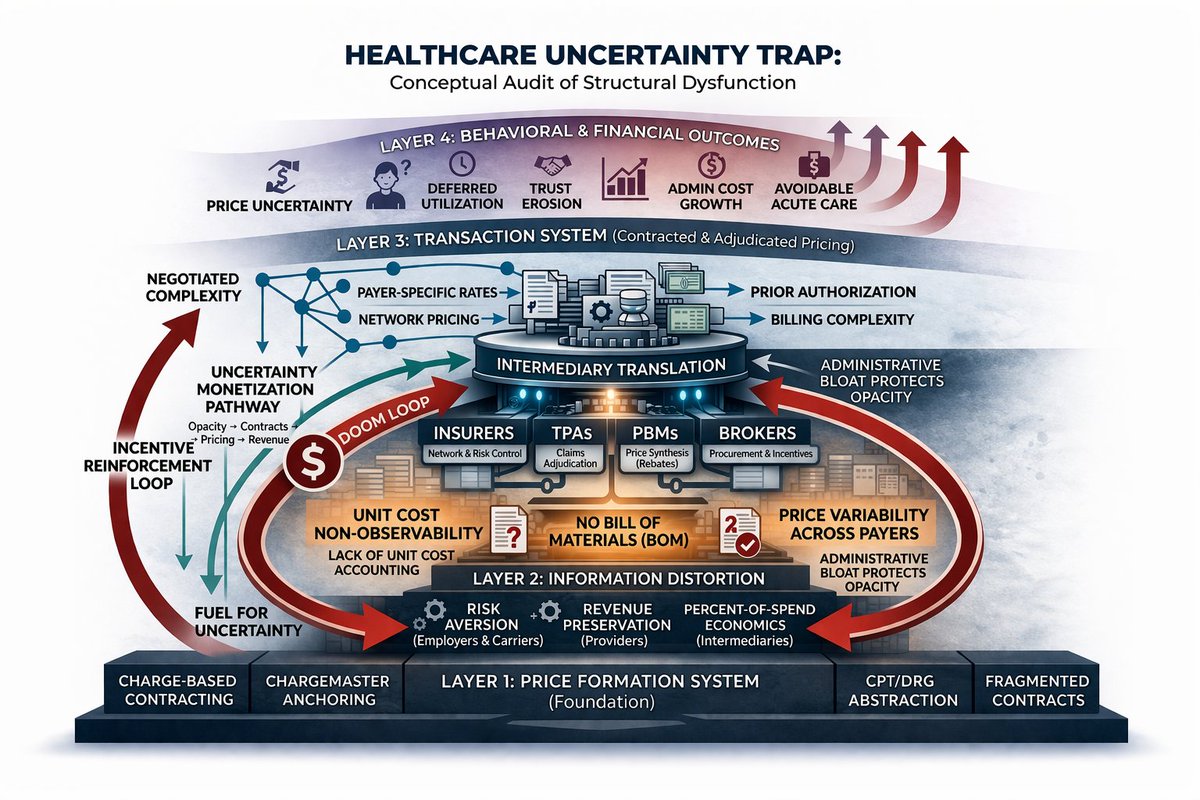
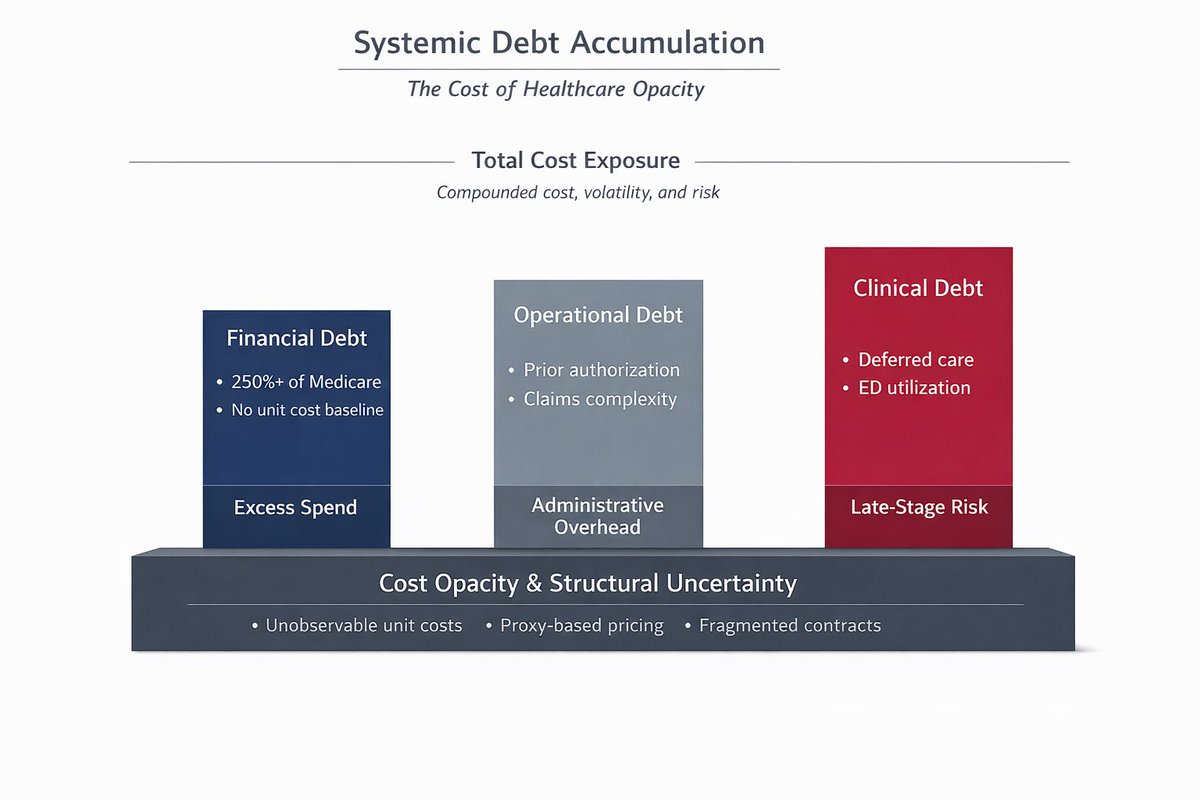
They build as three forms of structural debt:
1) Financial Debt
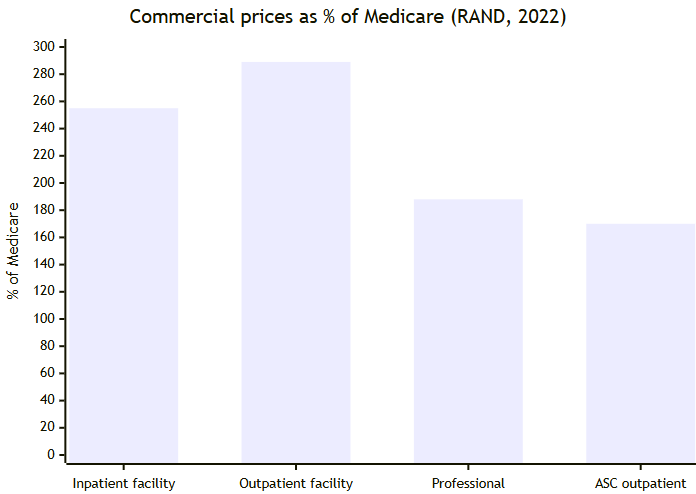
Employers pay 250%+ of Medicare without a unit cost baseline. That spread reflects pricing without cost visibility.
2) Operational Debt
The system runs on prior authorization, billing rules, and network design. These are the processing layers required to manage price uncertainty.
3) Clinical Debt
Uncertain costs shape behavior.
Care gets delayed.
Utilization shifts to higher-acuity settings.
Risk increases over time.
These liabilities sit in parallel, and originate from the same foundation:
Cost opacity.
Carrier changes and plan adjustments operate within this structure.
The leverage point is upstream:
Establish unit cost visibility.
Replace proxy pricing.
Constrain administrative processing layers.
Employers are financing accumulated exposure.
English