پن کیا گیا ٹویٹ

We’re live.
PepTracker is now available on the App Store.
Track your peptides, schedule injections, calculate doses, and log your protocols— all in one place.
📲 apps.apple.com/us/app/peptrac…
Coming soon to Android.
English
PepTracker App
124 posts
@PepTracker
The adherence layer for GLP-1s and peptide protocols. Download PepTracker ⬇️
Today, we took long-overdue action to restore science, accountability, and the rule of law. In September 2023, the Biden FDA pushed a number of peptides into Category 2 — “Bulk Drug Substances that Raise Significant Safety Risks” — driving a dangerous black market that puts Americans at risk. Now, after nominators withdrew 12 peptides, the FDA will remove them from Category 2 and will bring them to PCAC at its next two meetings, beginning in July—where independent experts will rigorously evaluate each substance on its scientific merits using full clinical, pharmacological, and safety evidence. • BPC-157 • Thymosin beta-4 fragment (LKKTETQ) • Epitalon • GHK-Cu (injectable) • MOTS-c • DSIP (Emideltide) • Dihexa Acetate • Ibutamoren Mesylate • Melanotan II • KPV • Semax (heptapeptide) • Cathelicidin LL-37 This action begins to restore regulated access and will immediately begin shifting demand away from the black market. We will follow the science, enforce the law, and deliver the clarity patients, providers, and pharmacies deserve.

GLP-1’s don’t simply cause you to eat less. They reduce inflammation, reduce cancer, improve arthritis pain, reduce alcohol consumption, protect the heart independent of weight loss, stimulate beta cells in the pancreas, keep you from developing type 2, and generally reduce all cause mortality. 😮💨 So no, you can’t just “eat less” and get the same benefits.

🚨 BREAKING: FDA APPROVES ELI LILLY GLP-1 PILL $LLY $NVO $HIMS
Expect a massive surge in compounding pharmacies, explicit warning labels on gray market peptides (currently is “not for human use”… ) and steep penalties for any venue besides Lilly selling Retatrutide. And per prediction, NIH budget to be increased 1%. More on that soon…
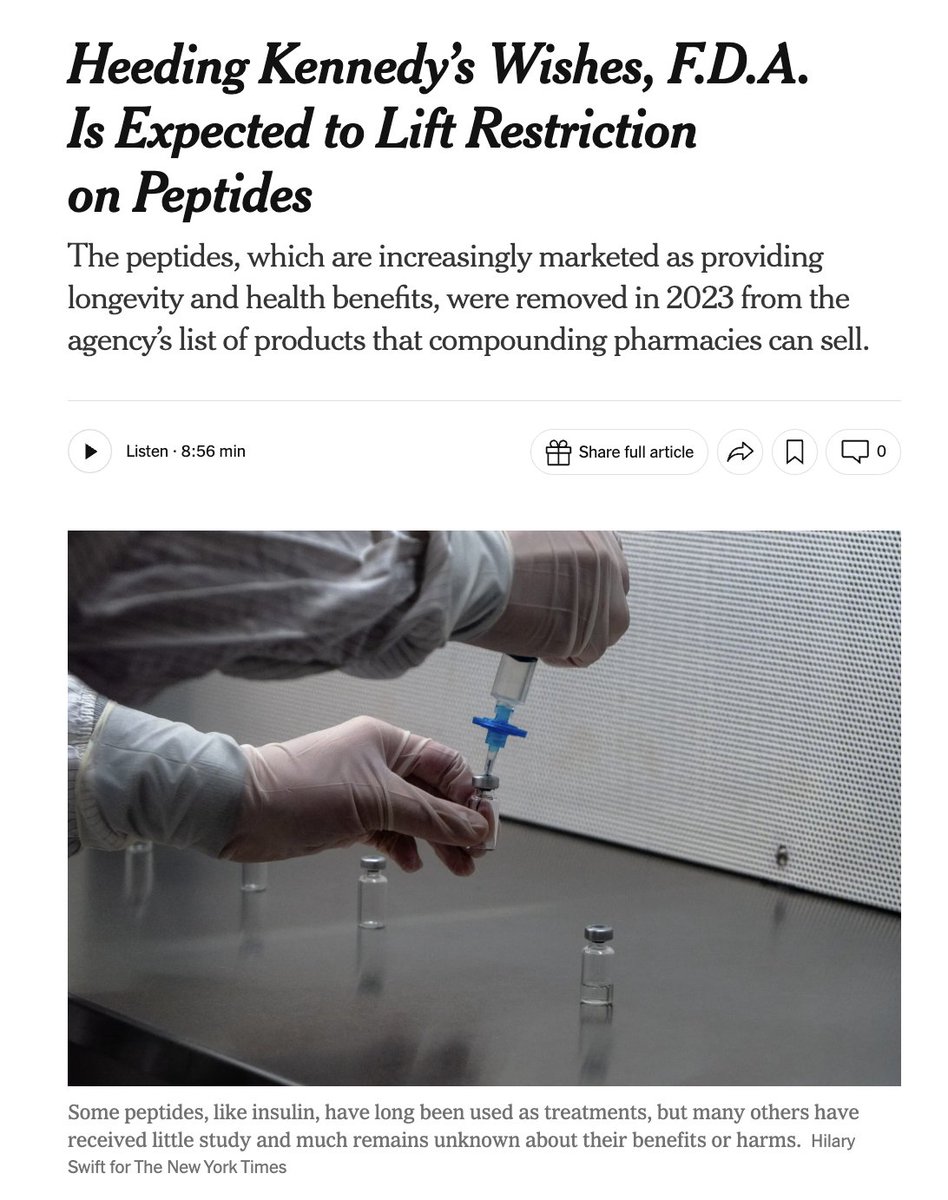
🚨 BREAKING NEWS: RFK Jr. says ~14 of 19 banned peptides can be legally compounded again by US pharmacies within a few weeks. This will ensure Americans are getting "a good product… from ethical suppliers" vs. black market drug dealers that provide "substandard product" with serious safety risks. The 19 compounds on FDA’s Category 2 compounding safety list include: • BPC-157 • Cathelicidin LL-37 • Emideltide (DSIP) • Epitalon • GHK-Cu (injectable) • GHRP-2 (injectable/nasal) • GHRP-6 • Ipamorelin acetate • Kisspeptin-10 • KPV • Melanotan II • PEG-MGF (pegylated Mechano Growth Factor) • MOTS-C • Semax • Thymosin beta-4 fragment (LKKTETQ) • AOD-9604 • CJC-1295 • Selank acetate (TP-7) • Thymosin-alpha 1 (Ta1) The five least likely to be legalized in a policy shift would be those with the most troubling safety signals or the weakest human data — for example: Melanotan II, Cathelicidin LL-37, GHRP-2, Ipamorelin acetate, and CJC-1295 — because of documented serious adverse events or other red flags in FDA’s risk assessment.
In a head-to-head type 2 diabetes trial, our investigational GLP-1 pill delivered superior blood sugar control and weight loss compared to another GLP-1. Detailed results were published today in The Lancet. Read more: e.lilly/4l1TTJS


