Cornelius Sendagire, MD retweetet

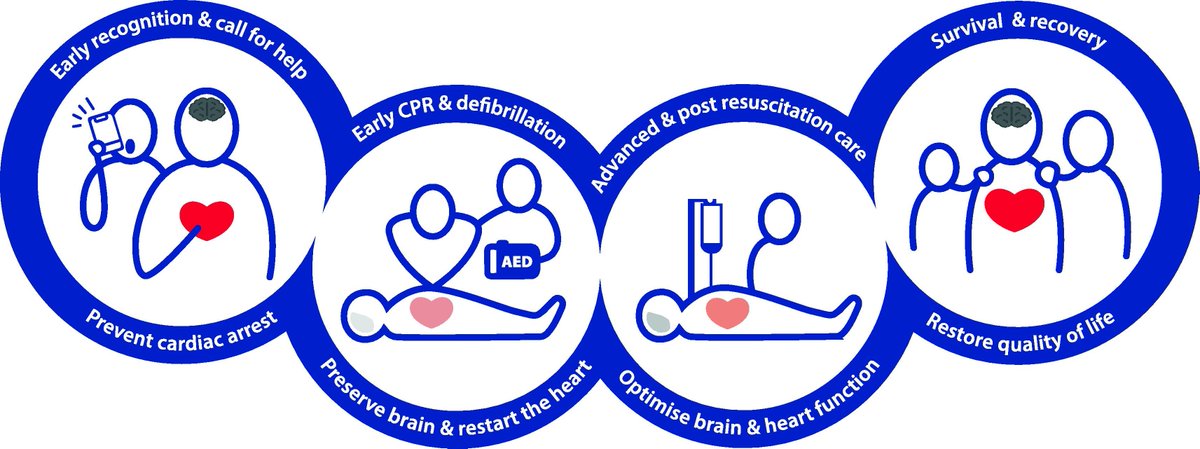
The 2025 European Resuscitation Council Guidelines have been released
All 11 plus the executive summary included below
CCR Journal Watch
criticalcarereviews.com/latest-evidenc…
English
Cornelius Sendagire, MD
1.3K posts

@cornels77
Cardiac anesthesiologist | Intensivist • Founder, Africa’s first Hypoxia Lab • Scalable ICU systems in Africa • Global Health • Medical Simulationist