G.W. Jackston@galactiator
$IBRX
In QUILT-3.055, if the overall ~14.1 month median overall survival (mOS) is the real story, why did the trial protocol (NCT03228667) prospectively list overall survival (OS) prolongation by ALC response as a co-primary endpoint?
Focusing heavily on the pooled~14.1 month mOS from the QUILT-3.055 trial and the early-stopped Lung-MAP S1800D abstract to claim Anktiva “adds nothing” in non-small cell lung cancer (NSCLC) misses the actual study designs and the FDA’s established standards for accelerated approval.
QUILT-3.055: a single-arm Phase 2b trial in heavily pretreated, checkpoint-resistant NSCLC. Every patient received Anktiva plus the same checkpoint inhibitor they had previously failed (true rechallenge setting). The cited overall mOS of ~14.1 months is the average across all participants, including both responders and non-responders.
The trial’s actual co-primary endpoint, defined in the protocol from the start, was OS prolongation by ALC response (achieving/maintaining mean on-treatment ALC ≥1,000 cells/µL). The mature January 2026 data cut showed:
* 77% of patients were ALC responders
* Responders lived a median of 16.2 months (hazard ratio 0.52, p=0.0369)
* Patients reaching even higher counts (≥1,200 cells/µL) lived a median of 21.1 months (hazard ratio 0.33, p=0.0009).
In plain terms, 77% of patients who restored their lymphocyte counts lived substantially longer, with those restoring them to higher levels lived even longer. Responders had roughly half the risk of dying at any given time compared to non-responders, a strong, statistically significant survival benefit. These results meaningfully exceed historical benchmarks of 7-9 months in this refractory setting. The 23% non-responders simply pulled the pooled average down, exactly what one would expect when testing whether Anktiva’s IL-15 superagonist mechanism actually improves outcomes.
The Phase 3 combo change does not “reset everything.” Companies routinely refine regimens during development, especially under RMAT guidance. The surrogate (ALC recovery) remains valid for the broader lymphopenia reversal indication, which is tumor-agnostic.
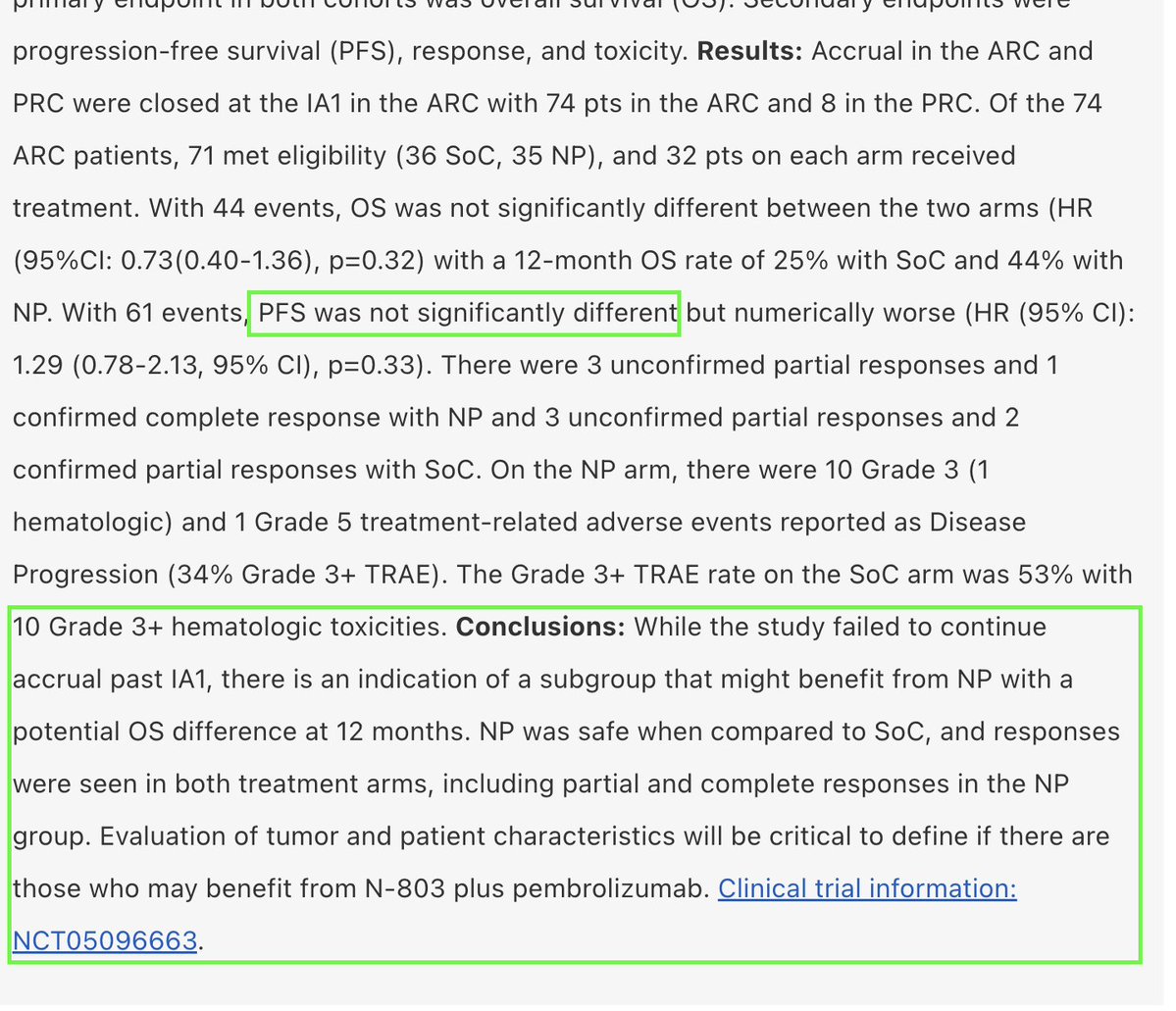
Lung-MAP S1800D: a randomized Phase II/III trial tested Anktiva + pembrolizumab versus standard chemotherapy in a randomized setting. Stopped early for futility on the primary endpoint, a legitimate data point. However, the full abstract’s conclusion (the portion cropped out in the screenshot in the thread) reads:
"While the study failed to continue accrual past IA1, there is an indication of a subgroup that might benefit from NP (Anktiva + pembrolizumab) with a potential OS difference at 12 months. NP was safe when compared to SoC, and responses were seen in both treatment arms, including partial and complete responses in the NP group. Evaluation of tumor and patient characteristics will be critical to define if there are those who may benefit from N-803 plus pembrolizumab."
Simply put, even though the trial stopped early for futility and did not reach statistical significance (HR 0.73, p=0.32), the authors noted a meaningful numerical improvement in 12-month survival: 44% alive with Anktiva + pembrolizumab versus 25% on standard chemotherapy. They explicitly called for better patient selection- exactly the type of insight the prospective ALC analysis in QUILT-3.055 delivers. Safety was also better on the Anktiva arm (34% vs 53% severe side effects), with tumor responses, including a complete response, observed.
The two trials asked different questions: QUILT-3.055 tested whether immune restoration correlates with survival; Lung-MAP tested a fixed combination against chemotherapy. One delivered a statistically significant, pre-specified surrogate signal; the other did not meet its bar for broad use. Neither erases the other.
The distinction is central to accelerated approval. The FDA allows approval based on a surrogate that is “reasonably likely” to predict clinical benefit in serious conditions with high unmet need (so patients do not have to wait years for large randomized survival studies). Here, the surrogate is reversal of chemotherapy-induced lymphopenia. The prospective ALC-survival correlation in QUILT-3.055, backed by Anktiva’s clear IL-15 mechanism, fits the FDA’s criteria. That is why RMAT designation (Feb 2025) and Expanded Access (June 2025) were granted for lymphopenia reversal across solid tumors.
This is the same Accelerated Approval playbook that let $MRK Merck Keytruda reach melanoma patients in 2014 on Phase 1 response rates, with large confirmatory survival data collected afterward. @ImmunityBio is following that path: BLA discussions for the lymphopenia indication are expected in second half 2026, with confirmatory randomized trials (including ResQ201A) to follow.
Cherry-picking the pooled mOS from one study while omitting the authors’ own subgroup nuance from another does not present a complete picture. Patients suffering chemotherapy-induced lymphopenia deserve the same consistent regulatory standards Merck received with Keytruda: surrogate first, confirmatory data second. The prospective evidence in QUILT-3.055 clearly meets that bar.
So while a lung-cancer-specific accelerated approval in the next 6-12 months is unlikely without stronger randomized data, a broader lymphopenia approval that includes lung cancer patients as part of the label is still very much on the table for 2H 2026 / early 2027.