
Marianne Chapleau
1.3K posts


Marianne Chapleau
@M_Chapleau
Neuropsychologist turned Medical Science Liaison. Passionate about patient care & improving the dx and tx of neurodegenerative diseases. Views are my own.
San Francisco, CA Bergabung Ocak 2020
958 Mengikuti2.4K Pengikut

@financedon2024 @vivekramaswami The implication that a man of color following a woman is suspicious or predatory… 🙃
English
@grinberg_t @UCSFmac @MayoClinic @gowoon_son @MayoPathology Congrats Lea! Enjoy the sunny Florida weather! ☀️
English

Big changes, new! After an incredible journey @UCSFmac, we’ve officially moved to @MayoClinic in Jacksonville, FL. The renovated lab is ready, and we’re excited to inaugurate it this Monday. Grateful to this amazing team—onward! @gowoon_son @MayoPathology

English
Big day for Life Molecular Imaging! 👏
investor.lantheus.com/news-releases/…
English
Marianne Chapleau me-retweet

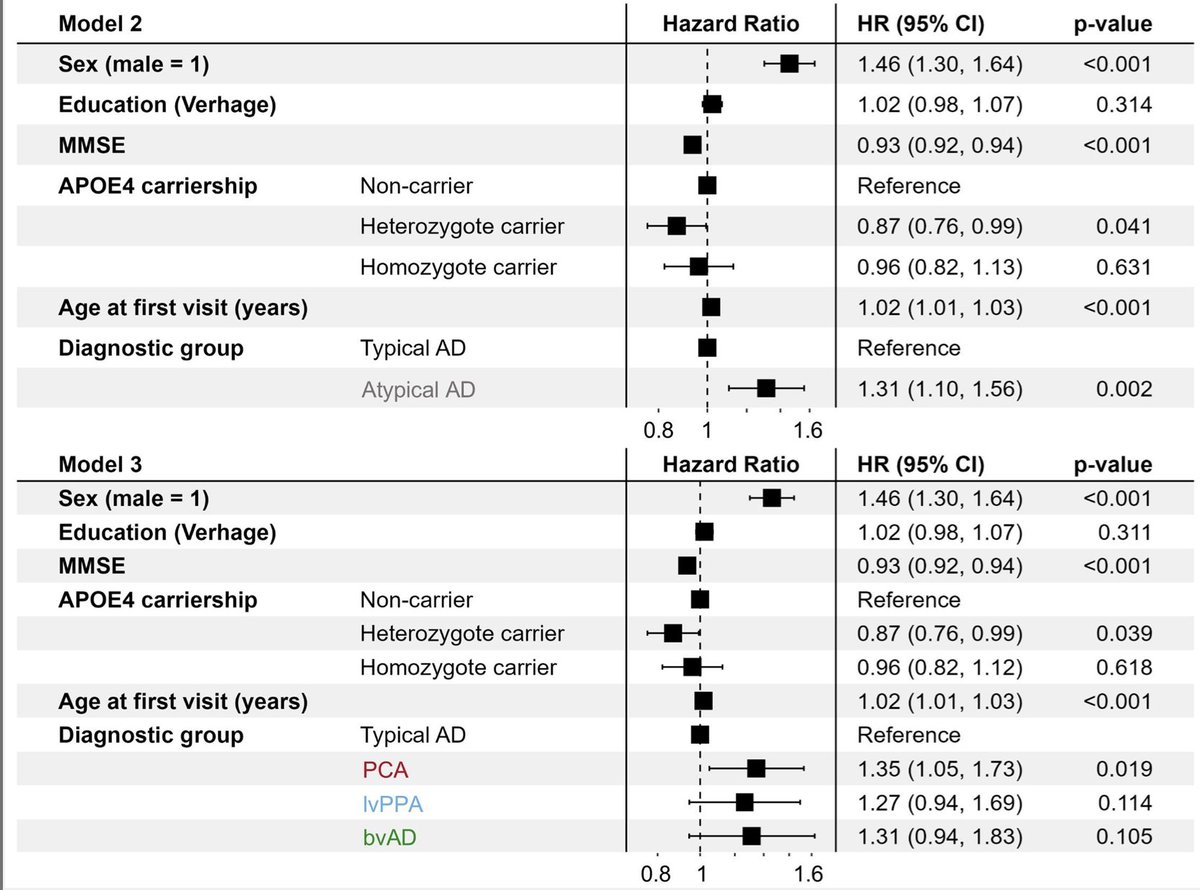
🚨NEW PREPRINT: An atypical phenotype is a risk factor for higher mortality in Alzheimer’s disease
@ilse_bader shows that an atypical (non-amnestic-predominant) clinical presentation is an important risk factor for mortality beyond age, sex, education, APOEε4-carriership and disease severity.
Link @medrxivpreprint: medrxiv.org/content/10.110…
@Colin__Groot @AlzheimerAms

English
Happy to share this great review on florbetaben, led by Aleksandar Jovalekic, highlighting its pivotal role in imaging Alzheimer’s pathology since its approval 10 years ago. Grateful to have collaborated on this work!
mdpi.com/1424-8247/17/1…
English
Marianne Chapleau me-retweet

📣 Postdoc Hiring📣
Join our project on how social health impacts cognition & resilience with a focus on women’s health
✅ Longitudinal data expertise
✅ Passion for aging research
✅ Team-oriented mindset
📍Karolinska Institutet 🇸🇪
💼 Apply now:
ki.varbi.com/en/what:job/jo…
English
Marianne Chapleau me-retweet

Massive paper alert: We performed extensive profiling of PI-2620 for 4R tauopathies. PI-2620 tau PET signals in PSP stem from neuronal and oligodendroglial tau, not astrocytes. Signals correlate with fibrillary tau, autoradiography, and autopsy data in PSP doi.org/10.1007/s00401…
English
Marianne Chapleau me-retweet

ARIA-E in Alzheimer disease is more likely in those with APOE ε4, microhemorrhages, low CSF Aβ42, and high Fazekas scores, but it does not generally worsen long-term cognition or function. ja.ma/4fOVui3

English
Exciting news for Alzheimer’s treatment in Europe! National decisions on access, pricing, and reimbursement are next, but this is a big step forward! 🎉
EU Medicines Agency@EMA_News
📢The CHMP recommends authorising a new treatment for early #AlzheimersDisease in the EU. Leqembi is intended for treatment of mild dementia and cognitive impairment in a restricted patient population with a specific genetic make-up. 👉 ema.europa.eu/en/news/leqemb…
English
Marianne Chapleau me-retweet
#CurePSP is now accepting applications for the Student Fellowship Program. This program supports students engaged in research on PSP and CBD, providing resources to drive meaningful advances in the field.
Deadline: January 31, 2025, by 5pm ET
psp.org/iwanttolearn/s…
#Research

English
Marianne Chapleau me-retweet
Study found frailty accelerates up to 9 years before dementia onset and is a key early marker. Frailty was linked to higher dementia risk even when measured years before dementia onset and may represent a target for prevention efforts.
ja.ma/4hLFake

English
Marianne Chapleau me-retweet

📢 Looking for a postdoc opportunity in neuroimaging research! 🎓 My focus: Alzheimer’s disease, cognitive aging, & functional networks. Skilled in multiple MRI modalities and neuropsych. Excited to connect with labs! #Postdoc #AlzheimersResearch #Neuroimaging
GIF
English
Marianne Chapleau me-retweet

Join us at #AAICAdvancements Exploring Equity in Diagnosis, Nov. 18-19 in Chicago and online! Be a part of the conversation around addressing disparities in an era of modernizing diagnosis for Alzheimer’s and other dementias. #ExploringEquity24 alz.org/exploringequity
English
Marianne Chapleau me-retweet

Whelp. Maybe a good time to mention that I am about to open a new PhD position in Sweden that just happens to be exactly four years in length. Any aspiring PhD candidates in neurodegenerative imaging or multiomics who want to "take a break" from the US, please get in touch!
English

Well said! And this framework does not diminish the importance of syndromic diagnosis or the quantification of clinical impairment.
Suzanne E Schindler@SuzanneESchind1
Having started my career in basic neuroscience research, I have always understood Alzheimer disease to mean the pathophysiology associated with amyloid plaques and tau tangles. As a clinician, I appreciate that the relationship between Alzheimer disease and cognitive impairment is complex. 1. Clinically diagnosing the cause of cognitive impairment is different than diagnosing that the patient has Alzheimer disease (pathology). Many of my patients with cognitive impairment have multiple diagnoses (e.g., sleep apnea, medication-related cognitive dysfunction, depression, previous cerebral infarction), and sometimes have Alzheimer disease (based on biomarker testing). I do what I can to mitigate the effects of all of these conditions, and when Alzheimer disease is present I do not assume that it is the sole or even the primary cause of cognitive impairment. This is true across multiple potential etiologies: for example, I may diagnose someone with cerebrovascular disease and a prior infarct based on MRI findings, but determine that this condition is asymptomatic and not contributing to their cognitive impairment. 2. Given the simplicity of some biomarker tests and the difficulty of clinical assessment, there is a risk that clinicians may diagnose the etiology of cognitive impairment as Alzheimer disease without doing a full work-up. This is why appropriate use recommendations for biomarkers always mandate that biomarker results must be integrated with a clinical evaluation and not used as a “stand-alone.” 3. Alzheimer disease pathology accumulates silently for ~10-20 years before the onset of cognitive impairment. However, during this pre-clinical phase the accumulation of amyloid pathology is associated with many other biomarker changes that appear pathological (e.g., abnormal CSF synaptic biomarkers, brain atrophy, brain hypometabolism). While the brain is remarkably resilient to damage and individuals may or may not develop symptoms, the brain is sick and the pre-clinical phase is a disease state. 4. Suggesting that a disease only exists when organs are severely damaged and failing (dementia) seems counter to what we have learned in other areas of medicine. For example, patients diagnosed with hypertension or asymptomatic coronary artery disease may change their diet and medications to avoid a heart attack. Individuals with asymptomatic chronic kidney disease may or may not go on to require dialysis, but they can be monitored and sometimes treated. 5. There are valid concerns about the stigma and risks of asymptomatic individuals being labeled as having Alzheimer disease given that they may or may not develop cognitive impairment. The solution is simple—we don’t perform biomarker testing in asymptomatic individuals outside of research studies or clinical trials. Again, this has been mandated by appropriate use recommendations for biomarkers. We can help patients by promoting accurate understanding and appropriate use of biomarkers. #EndAlz
English
@MilanNigam2 Pour attirer plus de psychologues dans le public, ça prend une meilleure rémunération… Les médecins sont biens au Québec 🙂
Français
@MilanNigam2 Quand j’ai obtenu mon diplôme en 2020, on nous obligeait, en tant que psys/neuropsys, à accepter un poste dans notre dernier milieu de stage si l’opportunité se présentait. La plupart trouvaient une excuse pour y échapper, car le salaire de base dans le public était de 66 000$.
Français

Je ne suis pas contre. Allez vous faire la même chose pour les IPS, Physiothérapeutes et psychologues? Je l'espère.
Christian Dubé@cdube2026
On doit améliorer l’accès et renforcer notre réseau public. C’est pourquoi on a l’intention de déposer un projet de loi qui ferait en sorte que les nouveaux médecins formés au Québec pratiqueraient dans le réseau public québécois durant les premières années après leurs études.
Français

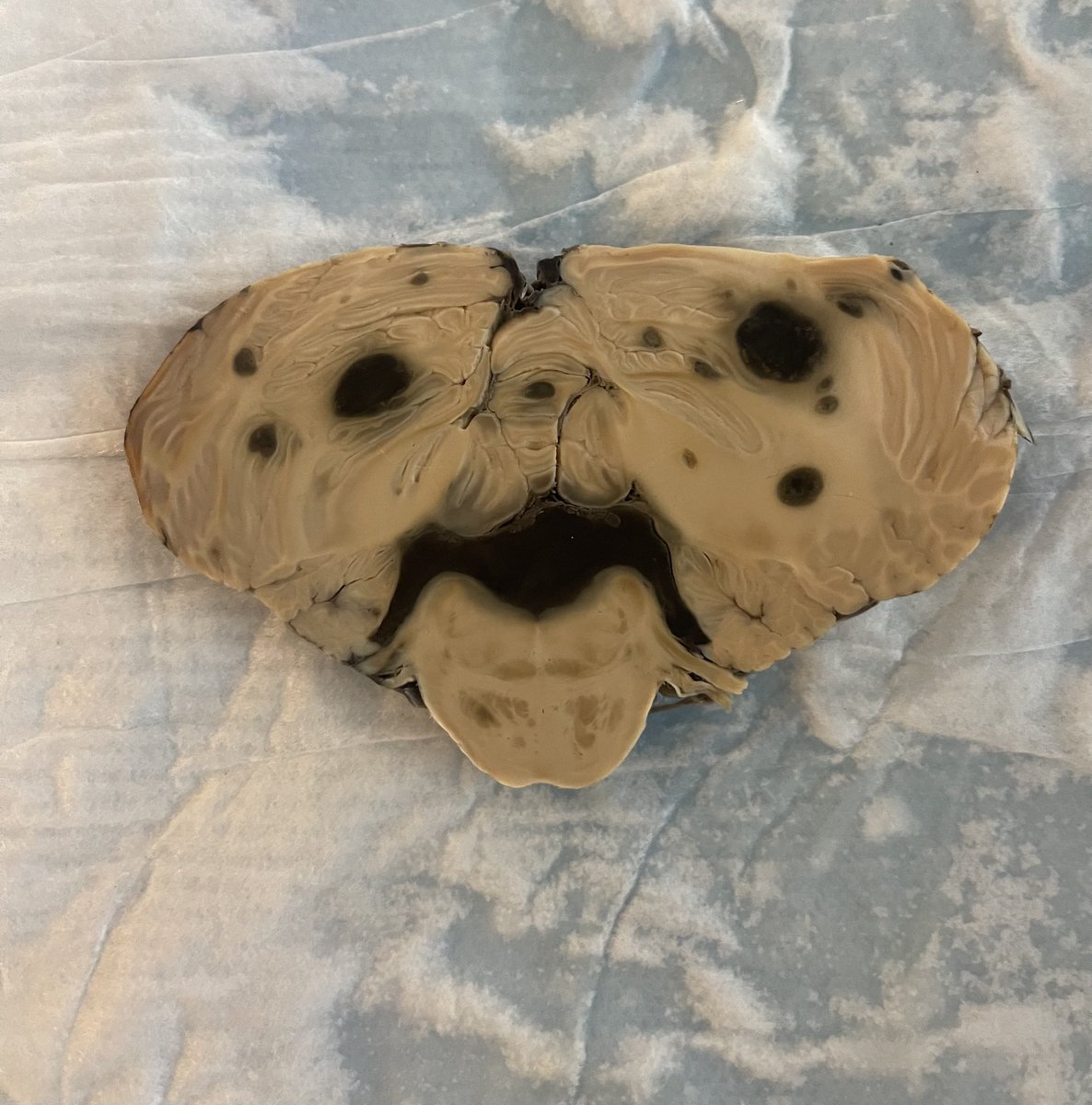
Sometimes we see things we don’t expect in our specimens! #neuropath #pathology #neuroanatomy #neurology #neuroscience 🤓🧠

English