Gu, MD がリツイート

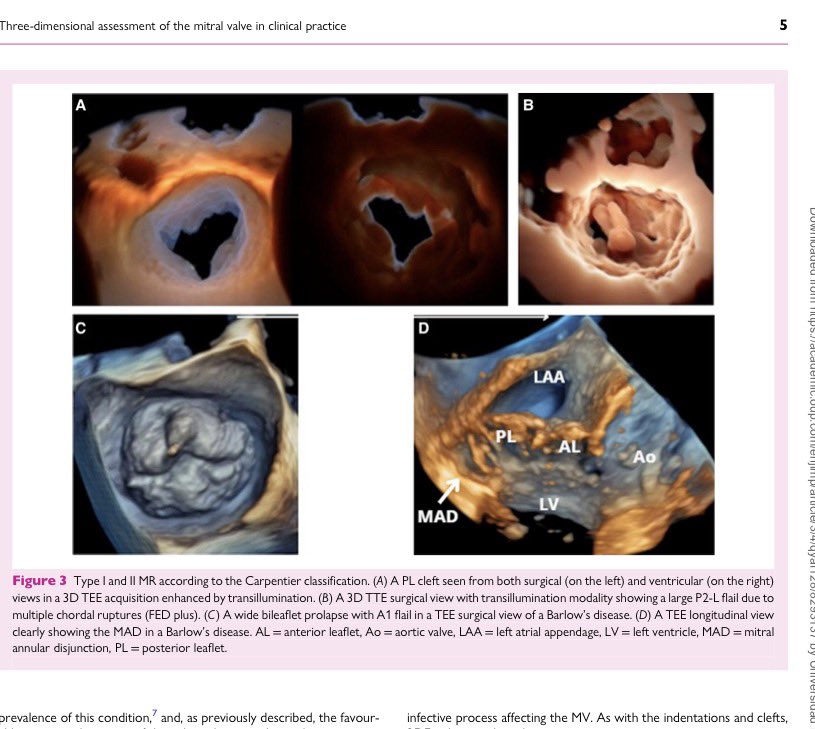
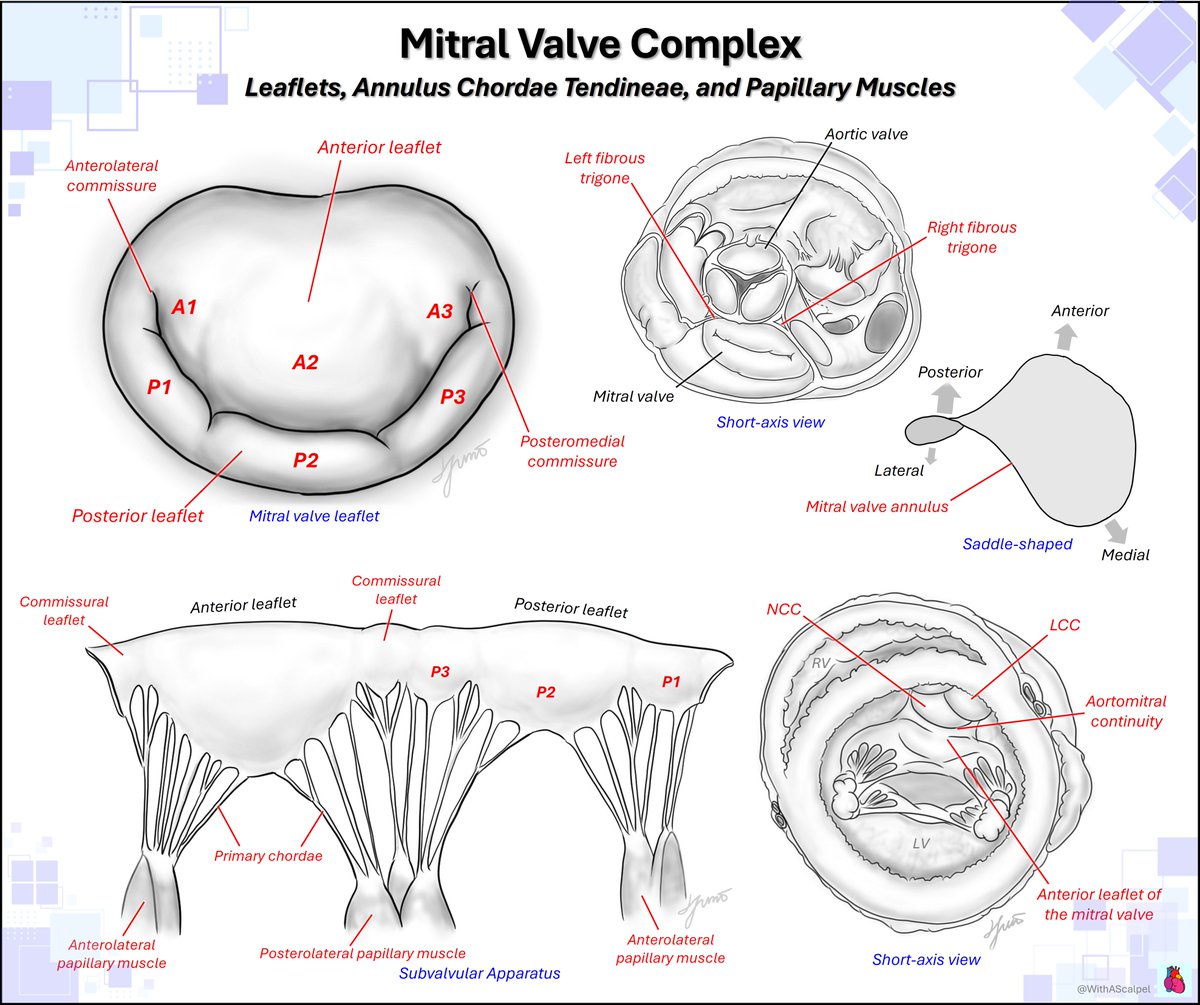
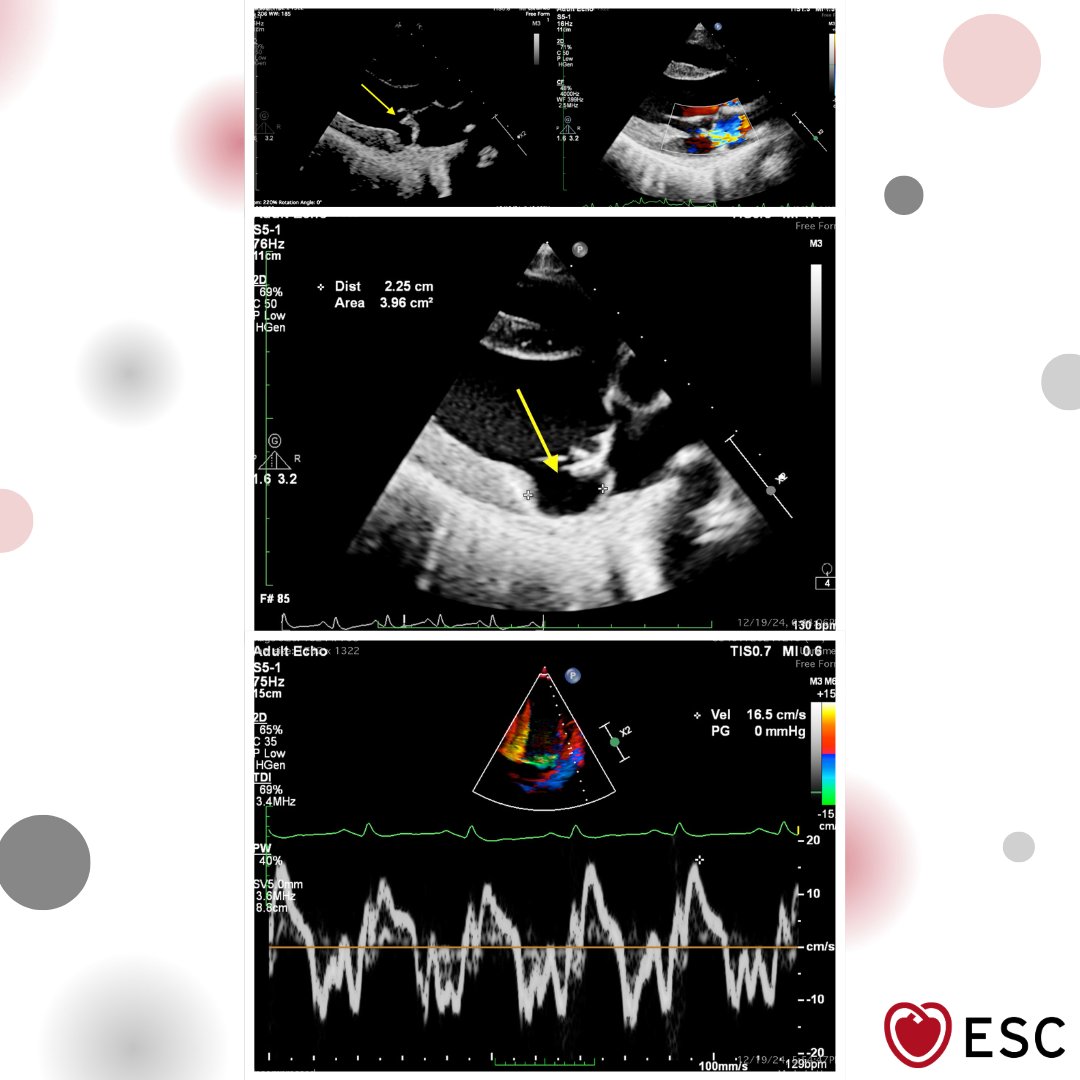
#ImageOfTheWeek by Avishkar Agrawal, Sumit Kumar, and Souvik Sardar from All India Institute of Medical Sciences, New Delhi, India A 28-year-old woman with mitral valve prolapse.
What additional high-risk echo finding may be present? ow.ly/V7iS50YJNIU
English