Elaine Francis 리트윗함

Only 10-15% of workforce training transfers to workplace practice: what we can do about it.
Recent research asserts that only 10-15% of what people learn in formal training actually transfers to workplace practice. Those of us building skills for improvement and change in health and care can relate to this. Health and care organisations invest massively in improvement training, yet it frequently fails to translate into practical improvements in care delivery.
The transfer problem is not primarily about the training itself or participant capability. The work environment is the primary determinant of whether learning transfers successfully. We, as leaders, hold the key to unlocking the 85-90% of learning that currently fails to translate into improved care.
Actions we can take to enable learning transfer from improvement training based on research findings:
1) Create explicit support structures. Improvement training participants need identified peer supporters and line managers who understand their role in enabling application of new skills. This support directly affects transfer through impact on motivation and determination to overcome obstacles.
2) Align learning with organisational priorities. When we connect improvement training and individual learning goals explicitly to strategic goals and health and care outcomes, we get more learning transfer.
3) Provide time and opportunity to apply learning. The research identifies availability of time, resources and opportunities to apply new knowledge as critical environmental factors. Improvement work needs protected space, not an expectation it will happen alongside unchanged operational demands.
4) Bridge the "knowing/doing" gap through transfer projects that address genuine organisational problems. These projects should be strategically aligned, adequately resourced and accompanied by clear agreements about outcomes between leaders and participants.
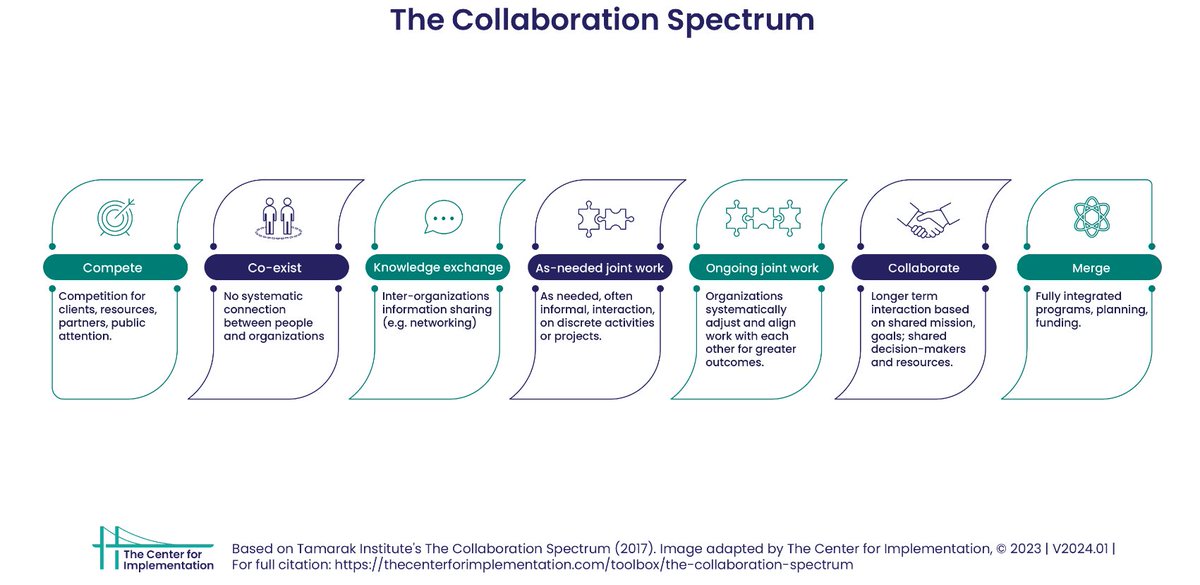
5) Foster knowledge networks and social exchange. Over half of participants change their knowledge networks after training, actively seeking expertise from experienced colleagues. We should recognise and enable these networks, creating conditions for knowledge sharing through communities of practice and regular opportunities for peer exchange.
6) Build a positive error culture. A culture that allows experimentation without fear of blame is both a predictor of informal learning and a facilitator of transfer. Improvement requires testing changes and testing requires psychological safety to learn from what does not work as well as what does.
7) Move evaluation beyond end-of-course feedback to assess behavioural change and organisational results. We should track whether participants are applying improvement methods, whether teams are adopting new approaches and whether changes are producing better care outcomes.
8) Integrate three forms of learning. Combine formal improvement training with informal learning through experimentation and reflection, and self-regulated learning where people set their own goals and monitor their progress. We should support individual learning journeys rather than treating training as a one-off event.
The evidence is clear: successful learning transfer is a system property, not an individual responsibility. When we create the environmental conditions that enable transfer, improvement training can fulfil its potential to transform care for the people and communities we serve.
#abstract" target="_blank" rel="nofollow noopener">tandfonline.com/doi/full/10.10… By Simone Kauffeld and colleagues. Sourced via John Whitfield.

English