Sabitlenmiş Tweet

Thanks @CureMelanoma for the opportunity to discuss ctDNA in #melanoma, also thanks to my son Auguste for the #cameo appearance!
Chicago, IL 🇺🇸 English
Alan Tan
3.5K posts

@alantanmd
Genitourinary Oncology, Associate Professor, Vanderbilt University Vice President, MRD Research and Clincal Strategy, Tempus AI

🧬 Ultrasensitive #ctDNA detection predicts early RCC recurrence after nephrectomy. Dr. Amaral & Dr. @alantanmd used NeXT Personal® to monitor high-risk localized kidney cancer post-nephrectomy: ✅ All ctDNA-negative patients stayed disease-free during follow-up. ✅ Every recurrence caught ahead of radiologic detection. ✅ 67% of initial detections were sub-20 PPM. Low-shedding tumors benefit from the use of ultrasensitive ctDNA testing technology. #PrecisionOncology #PersonalizedMedicine #KidneyCancer #ASCO #ASCOGU #RCC #RenalCellCarcinoma



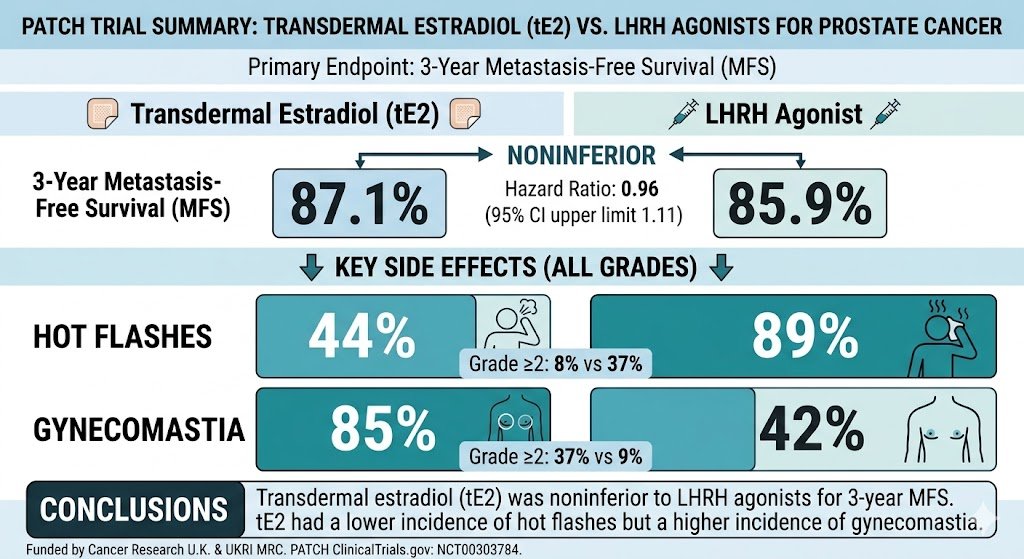
Was just wondering about uptake of this. We often encounter the dilemma of men wanting to treat their prostate cancer, but declining ADT for various reasons - namely short/long-term side effects - and desperately in search of alternatives. Better safety and financial toxicity profiles of tE2 are certainly noteworthy. @OncHahn @davidjeinstein @anis_a_hamid @DrRanaMcKay @ChrisSweens1 @PBarataMD @Uromigos thoughts on tE2?
Join our expert panel to explore evolving treatment sequencing in Advanced RCC. Discover insights on frontline decisions, adjuvant strategies & toxicity management to support long-term patient care. Watch the series today: hubs.li/Q047N0_F0 @montypal @cityofhope @DrVaishampayan @UMichMedSchool @alantanmd @VUMCDiscoveries








🎥 New interview with Dr. @alantanmd & Dr. @mm_zerey on breakthrough #UrothelialCarcinoma results! The study used NeXT Personal® to explore #ctDNA clearance as a biomarker for Enfortumab Vedotin + Pembrolizumab response: ✅100% baseline ctDNA detection (n=18). ✅88% clearance in non-metastatic pts (median 2 cycles). ✅40% clearance in metastatic pts (median 3.5 cycles). ✅Clearance = longer PFS (8 vs 6.8 months). ctDNA clearance correlates with clinical response and could guide treatment de-escalation.💪 Watch the full interview. 👇 #PrecisionOncology #BladderCancer #ASCOGU


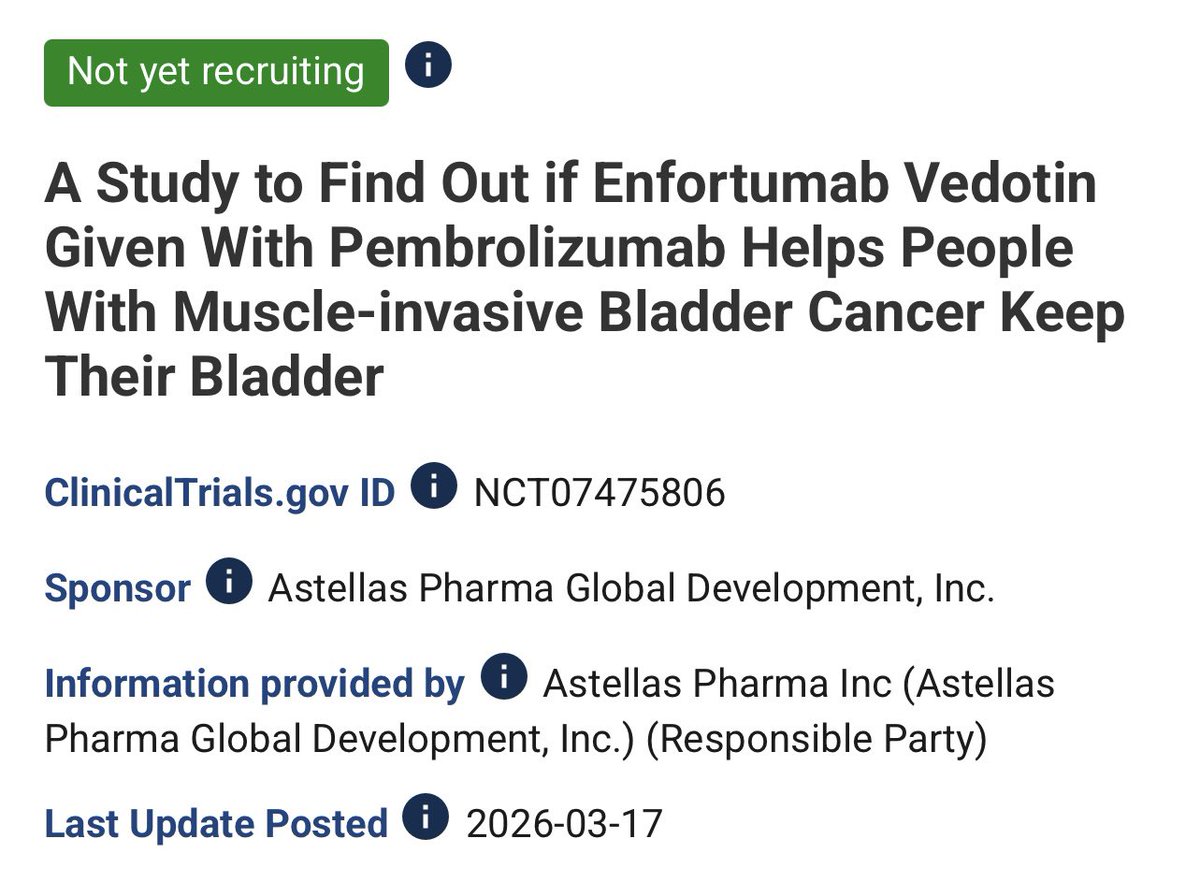
A 240 pateint single arm trial exploring 9 cycles of EVP without planned surgery in MIBC. This will answer the key questions ‘What happens if we don’t do cystectomy in those with clinical complete response after initial EVP’.It assesses cCR rates and bladder intact EFS. It will clarify ‘EVP 1st ask questions later’ #GUtrendingTopics @OncoAlert