Amy Andersen, MD retweetledi

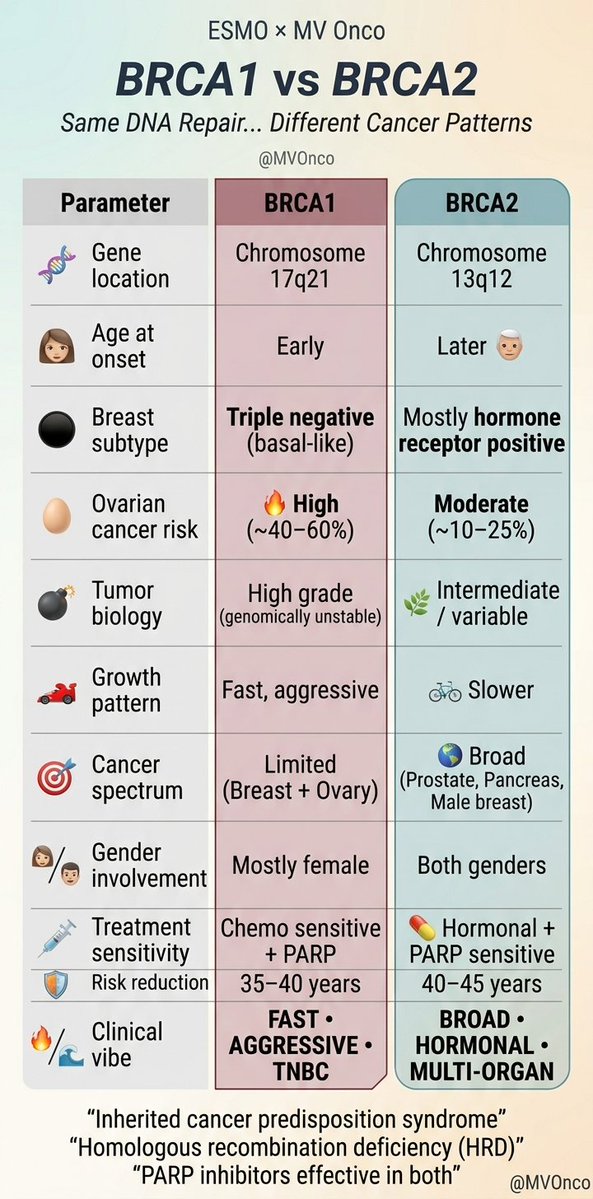
BRCA1 vs BRCA2 — simplified
• BRCA1 → early, TNBC, ovarian risk ↑, aggressive
• BRCA2 → HR+, broader cancers (prostate, pancreas)
• Both → PARP sensitive
Know the pattern → guide screening & therapy
#MVOnco #BreastCancer #Oncology
English