KRAS inhibitors in NSCLC:
-G12Di: coming soon to meet a major unmet need — same activity in smokers vs never-smokers?
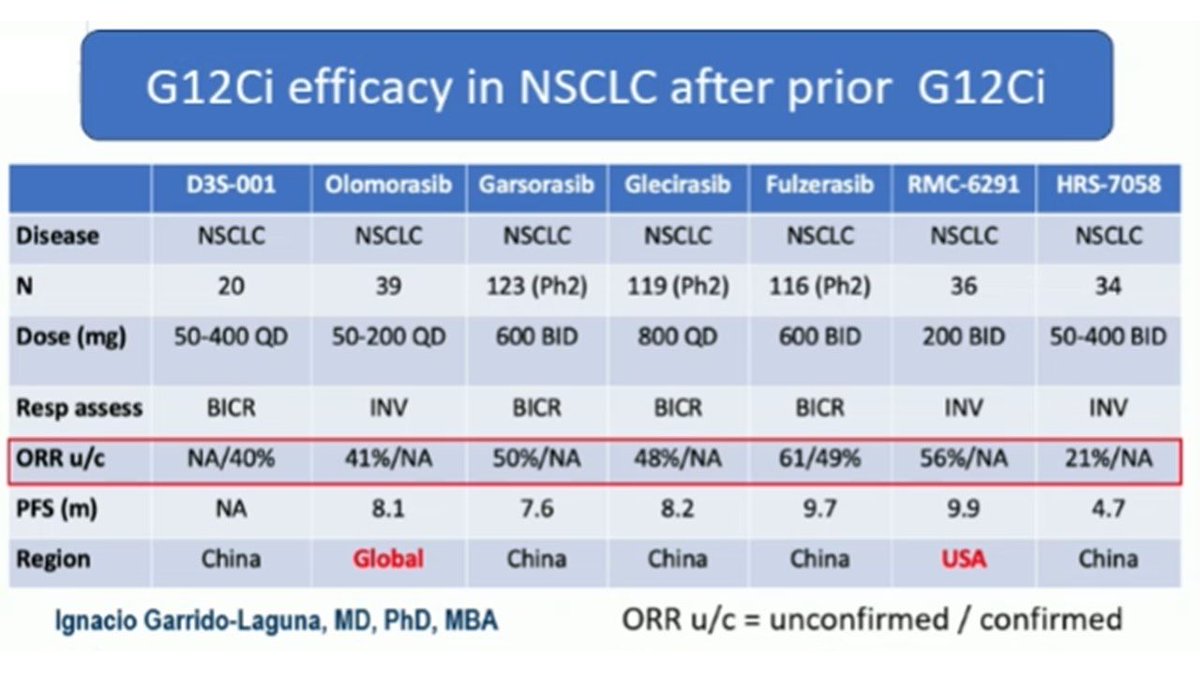
-G12Ci: expanding field, active in both naïve and post-sotorasib/adagrasib pts.
Excellent summary @GarridoLagunaMD #ESMO25



English