Bodhibrata Banerjee
133 posts

Bodhibrata Banerjee
@BodhibrataB
MD (Medicine) DM RHEUMATOLOGY SR, PGIMER,CHD SCE Rheumatology (RCP, UK) Member of SLEuro Healer, passion and love for Rheumatology
Kolkata, India Katılım Aralık 2022
243 Takip Edilen121 Takipçiler

This young lady presented to me with malar rash, oral sicca, Raynaud’s phenomenon, loss of facial fat, dry cough, and breathlessness. HRCT thorax showed ILD with a UIP pattern.
Her ANA IIF was positive, but anti-dsDNA was negative, complements were normal, anti-SSA/SSB were negative, and anti-U1RNP was negative. No other major organ involvement was noted.
However, ANA subserology revealed one strongly positive antibody.
Can you guess which antibody it was?
@docakx @IhabFathiSulima

English
Such a lovely analogy applied to our life also. Treat to target approach reminds me of the words of Confucius. In RA, the final outcome depends less on the initial drug and more on how consistently we adjust therapy to reach the target. The journey of life is like that too.

English
⭐ Occam's Razor vs Hickam's Dictum : Simplicity vs Complexity in Medicine

English

If a young patient’s back pain INSPIRES movement but hates rest, think inflammatory.
⭐ Remember the mnemonic "INSPIRE" for IBP

English




@Abhilasha21822 Congratulations madam.
Can you kindly share your key thoughts regarding importance of ANA blot testing in SLE?
English

Honoured to receive Second Prize at “Debates in Medicine” hosted by the Academy of Medical Sciences, Nagpur.
Debate Topic:
“ANA blot testing is not mandatory for diagnosis of Systemic Lupus Erythematosus.”
I spoke against the motion, advocating for a rational, evidence-based, and context-driven approach to ANA immunoblot interpretation in SLE.
In lupus, diagnostics are not about ordering more tests,
they are about ordering the right test, for the right patient, at the right time.
Grateful to the chairpersons, judges, and fellow speakers for an intellectually stimulating session and meaningful academic exchange.
#Rheumatology #SLE #ANATesting #Immunology #MedicalDebate #EvidenceBasedMedicine

English
@gurdeep_dulay @RheumNow Nowadays, anti-MCV antibodies are commercially available in certain labs. Testing for this antibody might help to rule out the other differentials like peripheral SpA, viral arthritis, CTD arthritis etc.
English


English

⭐ Danda Sign in Psoriatic Arthritis (Swelling of IP thumb)

English

🖐️ Your fingers can diagnose before your X-ray does.
Hand pain + swelling?
Touch first.
Feel second.
X-ray last.
🦴 BONY, hard, nodular joints
→ Think Hand Osteoarthritis (Heberden’s / Bouchard’s)
🧸 Soft, boggy, tender swelling
→ Think Inflammatory arthritis (RA, PsA, etc.)
This one bedside trick saves labs, saves time, saves misdiagnosis.
And the final judge?
📸 X-ray of Hand OA shows:🪽

English
@alb_giraldo @RheumJnl @OxfordJournals There is an antibody associated with GI dysmotility in SSc which is called anti-CDT. This highlights the fact that dysmotility is not only driven by fibrosis but also immune mediated injury to the nerve plexus.
English

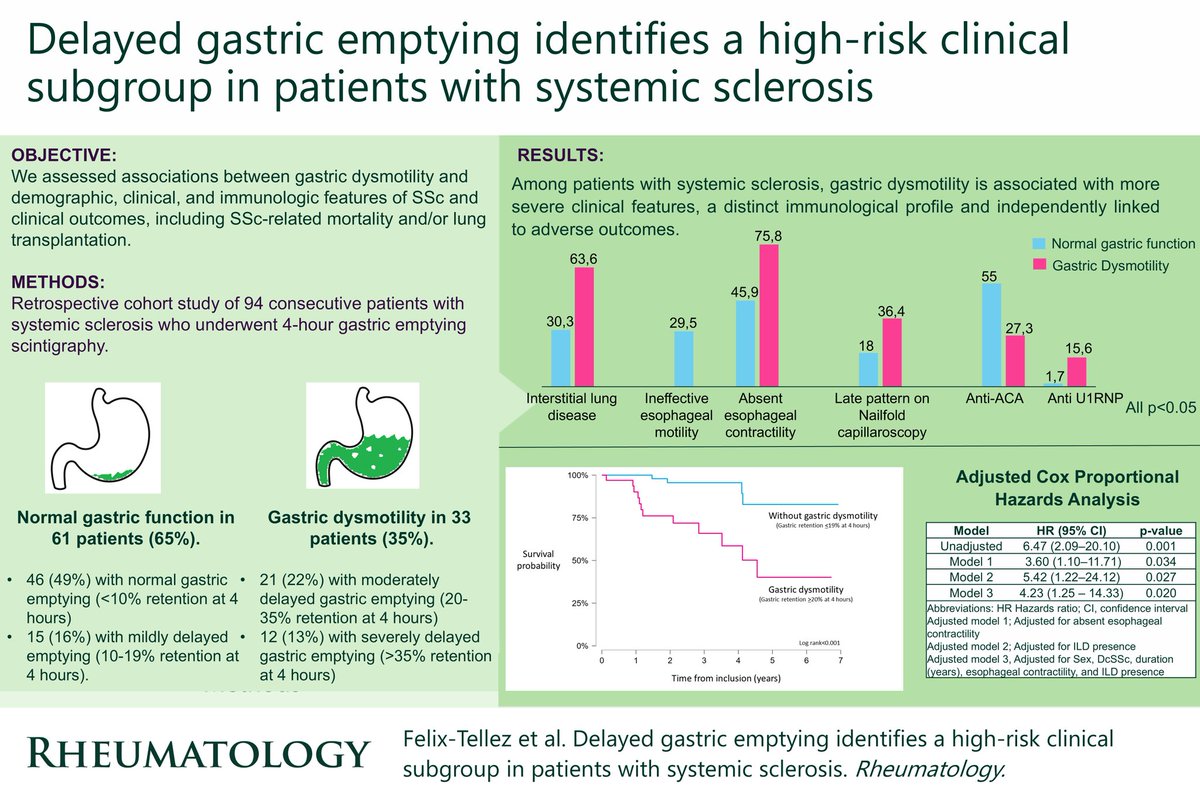
Gastric dysmotility identifies a high-risk systemic sclerosis (SSc) subgroup with more severe GI/pulmonary involvement and independently predicts serious outcomes, as demonstrated by the results of a recent cohort study:
◦ Prevalence: Gastric dysmotility present in 35% of 94 SSc patients (≥20% retention at 4 h scintigraphy)
◦ Clinical associations:
- Interstitial lung disease: 64% vs 30% (p = 0.033)
- Absent esophageal contractility: 76% vs 46% (p < 0.001)
◦ Serological associations:
- Less common with anti-centromere antibodies: 27% vs 55% (p = 0.009)
- More common with anti-U1RNP antibodies: 16% vs 2% (p = 0.011)
◦ Prognostic value (mean follow-up ~2.8 years):
- 17% reached SSc-related death or lung transplantation
- Gastric dysmotility strongly predicts adverse outcome:
• Unadjusted hazard ratio (HR) = 6.5 (95% CI 2.1–20.1, p = 0.001)
• Adjusted HR = 4.2 (95% CI 1.3–14.3, p = 0.020)
These findings underscore the importance of objective assessment of gastric function and its potential role in risk stratification in SSc patients.
*Felix-Tellez FA, Guillen-del-Castillo A, Pedroza C, et al. Delayed gastric emptying identifies a high-risk clinical subgroup in patients with systemic sclerosis. Rheumatology (Oxford). Published online February 6, 2026.
🔗doi.org/10.1093/rheuma…
English