
Medicine Investor
428 posts

Medicine Investor
@BuysideBiotech
L/S Healthcare. Not investment advice. Master of the Eephus.
Tiburón (MX: KOFL) Katılım Nisan 2020
1.7K Takip Edilen2.7K Takipçiler

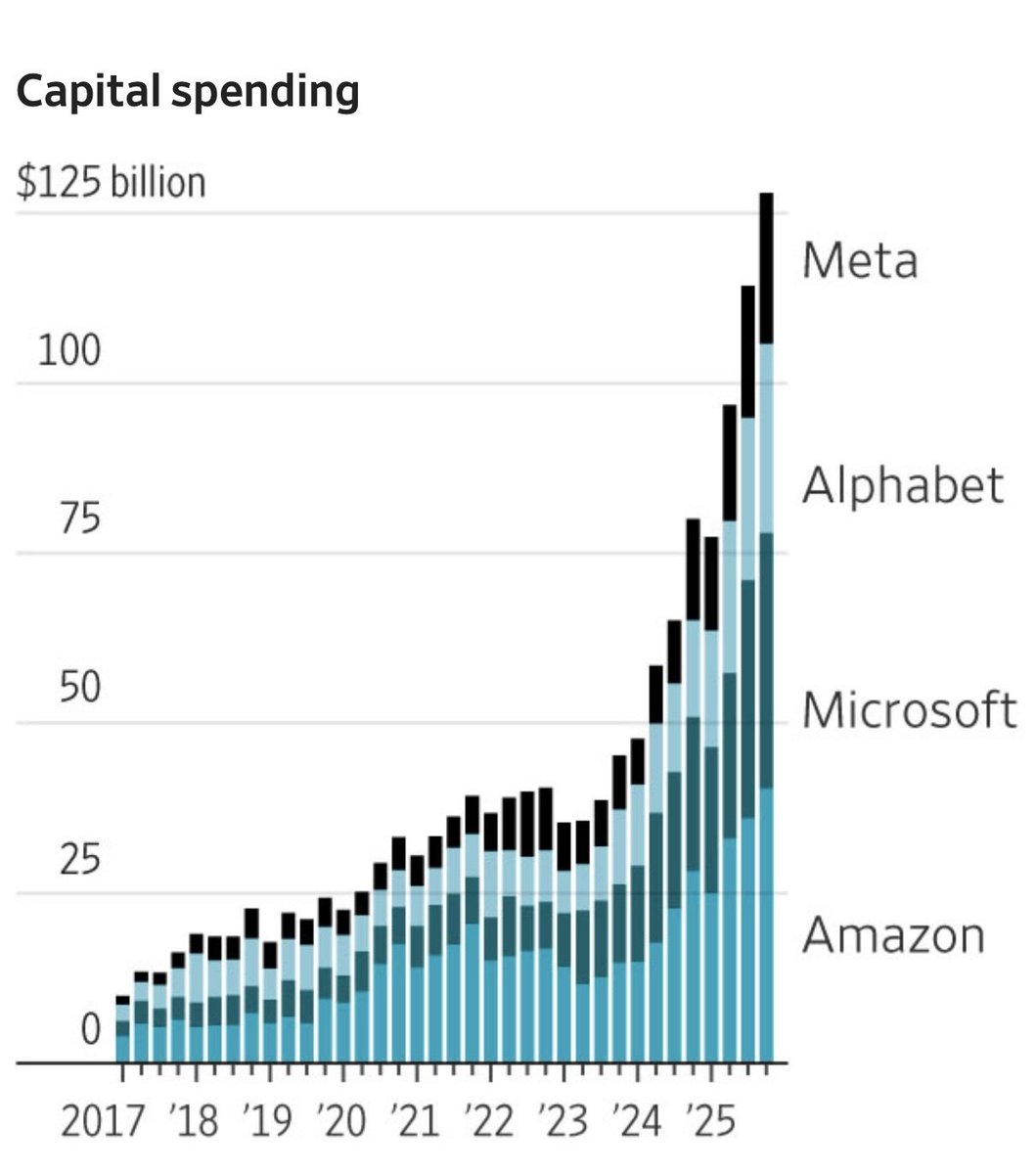
In a gold rush, sell picks and shovels
4 companies are investing $670B in data centers and AI infrastructure this year
The capital spending is 2nd only to the Louisiana Purchase which doubled the size of the U.S.
Electrical and Mechanical companies will be in high demand to construct these data centers
Invest in the trades
Sell picks and shovels

English
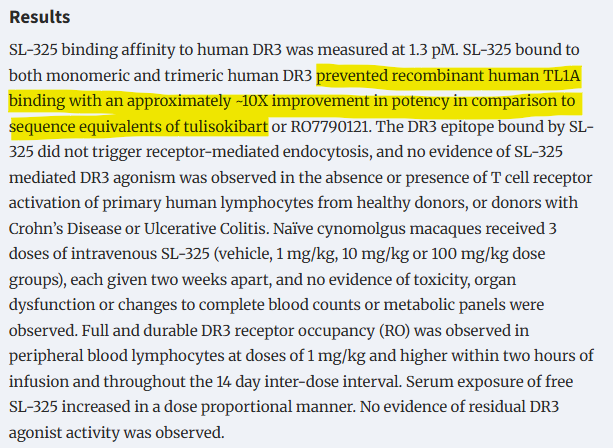
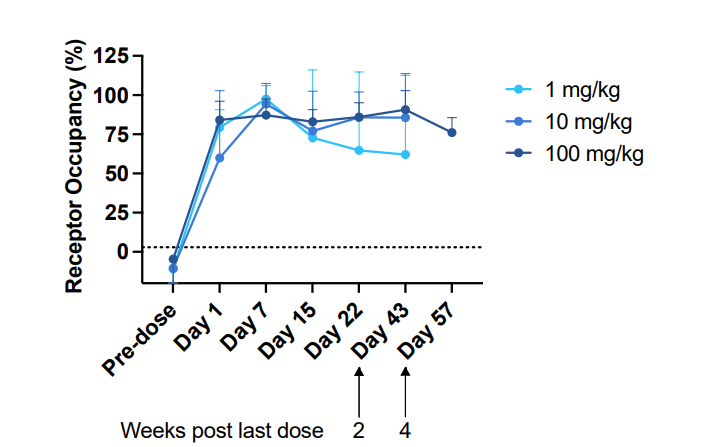
@Archimedes20311 Sure, ADAs pop up at lower trough concentrations based on NHP data
All that matters for the stock in the short term is RO and safety
English

@BuysideBiotech RO is also not how you want to do this imo. Drug levels matter a lot here especially since this isn't a serum ligand , tissue etc. which the RO assay is probably measuring
English
PD-1 like blockade of TL1A axis.... interesting $STTK
English

I actually like Shkreli although I am far from agreeing with him on many points. He at least has balls.
Which is not something I can say about many in our business.
And laughing about someone blowing up is a very bad karma. Markets are round and have a shape of a suitcase. eventually it will meet you on one of the corners.
Anders@Anders_Research
LOL Shkreli account completely wiped out by $CAPR Says he’s sorry “if anybody joined me on that” He also wants you to know that: 1) It’s no big deal (for him) 2) He is glad the account blew up 3) $QCLS, a nano-cap quantum-adjacent shell co he is advising, is the next move. 🧵
English
Like for near term data
$CDTX
$DRUG
$FULC
$TRVI
$PRAX
English


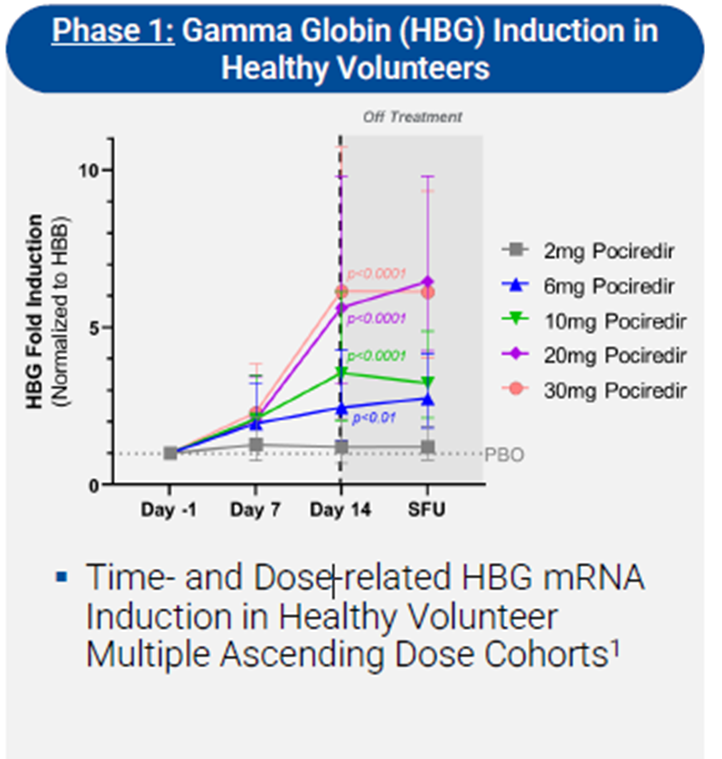
First, scientifically and mechanistically, there are lots of reasons to believe in the potential of $FULC's approach in SCD management.
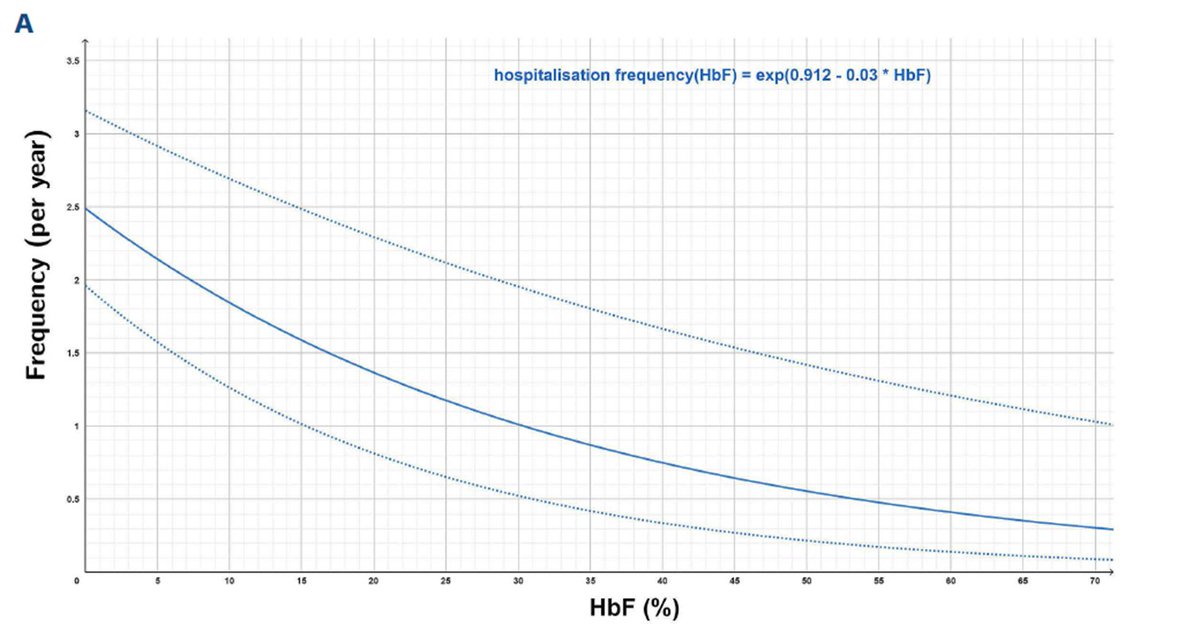
Higher levels HbF are beneficial in SCD because HbF inhibits the polymerization of HbS, which is the primary cause of red blood cell sickling and vaso-occlusive crises. Mechanistically, HbF does not participate in the hydrophobic interactions that lead to HbS polymer formation under deoxygenated conditions, thereby reducing intracellular HbS concentration and delaying or preventing sickling.
Clinical and genetic studies provide compelling evidence: patients with hereditary persistence of fetal hemoglobin or high HbF levels (≥20%) often exhibit milder disease phenotypes, with fewer pain crises and improved survival (Steinberg et al., 2014; Powars et al., 1984).


English
@SMB_Attorney Go buy a burger @SteaknShake
Price is a forward looking mechanism
English

Maybe I’m wrong?
If so, and there are actually legitimate uses for Bitcoin, please tell me concretely what you’ve used your Bitcoin for recently?
“Reserve currency” doesn’t count, I want actual transactions.
I’m all ears!
SMB Attorney@SMB_Attorney
At present, there is no legitimate use case for Bitcoin. Even if there is, 99% of holders don’t understand it and are holding as a pure speculative play. Making it still, even at $118k, susceptible to a spectacular collapse under the right circumstances.
English
@plainyogurt21 CDC has robust data. Majority of cases are (H1N1)pdm09 and H3N2 this season
English

@BuysideBiotech I think the FLU B strain was the one I picked as 10nM but if the EC50 is less than 1nM then makes sense why people think it’s a home run.
Do we have a composition for the current flu season?
English
Seeing some smart people long $cdtx. Fc-Zanamavir for Influenza prevention.
Severe flu season, proven drug, what's not to like?
Here's my question: Why doesn't the co show Concentrations for CD388 in epithelial tissue or nasopharyngeal swabs?
English
@plainyogurt21 Like the way youre looking at this @plainyogurt21 but EC50 for H5N1 is <1nM i believe. Also in this ballpark for relevant strains in circulation as it relates to the NAVIGATE trial $CDTX
English
Here's my rough math:
Fc Fusion protein serum vs lung concentration 5-20% based on 34% in mice (CD388), the prior data on Fc-AAT at lower range of 5-10%.
EC50 is between 1-10nM (cidara).
Molecular weight is 65 kDA for CD388.
Based on pharmacokinetics, Concentrations about 2 months form injection is ~10 ug/mL. Beep boop beep, plug into chatGPT, -> 150nM.
So 10% of 150 is 15 nM, slightly above the H5 N1 EC50 for CD388, doesn't seem like the sure thing I'm hearing about......
English
@punnettsqrcap Gotcha. Co has yet to share data on respiratory penetration. I remain skeptical.
English

@BuysideBiotech I’m saying the issue with the original drug wasn’t biodistribution, rather oral bioavailability. It works as IV in acute setting.
English
@punnettsqrcap conjugating the molecule only exacerbates the biodistribution issue w/ respect to lung penetration
English
@BuysideBiotech You are confusing oral bioavailability with biodistribution. Two very different things.
English
@Alexand80831564 You really think this chart looks great??
English

5yr $XBI chart looks great to me
Double bottom June ‘22 and Oct ‘23 with higher lows held in all of 2024
Mind blowing underperformance compared to $QQQ in same time period
$XBI +2%
$QQQ +137%
$IWM +37%
Still a ton of bio 5-10 baggers I’ve seen in this “lost” half a decade

English

Appreciate the open dialogue here
$AXSM traded up (alot!) on ph2 MDD results, $CMPS did not trade well following ph2 in TRD — why would it be different this go around? Expectations are for a replication of the ph2b…
Seems like they will have to prove that they commercially viable before the mkt respects it
English

1/2 $CMPS is a $300M MC 0EV stock <6mo from a P3 readout in TRD as the first-in-class psychedelics play. The P2b data shows a 15-pt MADRS drop with a clear dose response for 25mg vs 10mg vs 1mg. Treatment resistant depression (TRD) is a massive unmet need and $CMPS COMP360, if successful will be a $B+ drug. If approved, they would be second ever drug approved for TRD after $JNJ Esketamine/Spravato which is currently annualizing at $1B/year with a worse side effect profile (1/10 rate of vomiting) worse convenice profile (2x a week for first month, then 1x for month, then every two weeks) and a direct generic competitor (IV Ketamine clinics). $CMPS is potentially a quarterly medicine, without disscotion/vomiting that would be highly preferable.
Risks: there are four areas of pushback, first and foremost is mgmt.
Mgmt have not done a good job of either executing or guiding the street. They have pushed back the P3 twice, a total of 12 months. That said the data is now around the corner (2Q) and they are close to the finish line.
The second is IP. There is a (?lazy) stigma applied to companies without patents on composition of matter, that seems to just evaporate once the P3 comes out - $AXSM is a good example where pod analysts spent most of 2019 claiming a hokey mixture of an already approved antidepressant mixed with cough syrup was never going to fly as a successful drug for MDD. January 7th 2019 $AXSM was an $8 stock after their positive P2 in MDD, 6mo before their P3 they were at $24 and they closed that same year with an $87/share financing after their positive P3. Today they are $4B company with a strong launch in MDD. People also underestimate how often companies with no CoM IP get bought: $KRTX acquired by $BMY for $14B, $GWPH acquired for $7B by $JAZZ, $ZGNX acquired by $UCB for $2B and many more. MAPS (now Lykos) have made multiple attempts to invalidate the IP $CMPS which have all failed. The patent on the polymorph remains robust. If there was an easy way to go around it they would have likely done so. On top of which $CMPS have NCE exclusivity which is 7.5Ys (5Ys plus the stay or 2.5Ys) as an ultimate backstop.
The third area is suicidality. The the $CMPS P2b trial there were no suicides or attempted suicides. There were suicidal behaviors (harming yourself but not attempting to kill yourself) these were present across all groups 25mg 10mg and 1mg (1mg was the "placebo" given it is deemed sub therapeutic but was administered to minimize functional unblinding, more on this next) at rates of 3.7% 1.3% 1.3%. One important thing to point out is that all 3 of these patients with suicidal behaviors on 25mg of COMP360 were nonresponders. It is quite reasonable that if a person has TRD (i.e. is depressed and has also failed to respond to two different therapies already) and then fails to respond to what they may see as the last line therapy that they would be suicidal. It is obviously then no surprise that SPRAVATO, the only other treatment for TRD has a black box warning for suicidal thoughts and behaviors. What is more surprising is that essentially all antidepressants for MDD ("regular" depression) also have black box warnings including SSRIs (Prozac etc) SNRIs (Effexor etc) Tricyclics (Elavil) and others. Sadly people with depression are sometimes suicidal (the lifetime risk of a suicide attempt is 30% with MDD) people with TRD are between 2-10x more likely to attempt suicide vs MDD. $CMPS will get a black box for suicidality, just like every other antidepressant and it will not have any material effect on its prescription.
English