Sabitlenmiş Tweet

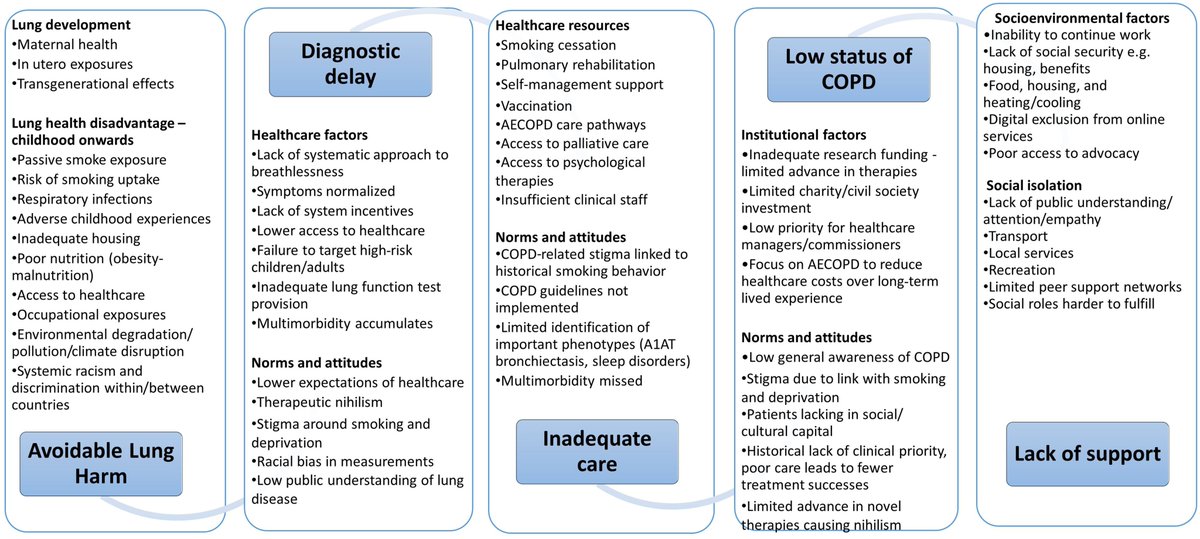
Lung Disease and Social Justice: COPD as a Manifestation of Structural Violence atsjournals.org/doi/full/10.11… @atscommunity @asthmalunguk @ATSBlueEditor /n
English
Nick Hopkinson
29.8K posts

@COPDdoc
Professor of Respiratory Medicine FRCP #COPD Tobacco control, social justice, lung health 🫁 🚭 #NHS Born at 323ppm.




Israeli authorities and security forces deliberately targeted Palestinian children, resulting in genocide, crimes against humanity and war crimes in Gaza, and war crimes in the occupied West Bank, an independent UN inquiry said reut.rs/4eD9CfA






A five-year-old was prescribed the wrong treatment after a breakdown in communication between healthcare professionals. Our investigation found failings at every stage and that better communication could have prevented this entirely. Read more: orlo.uk/XmzUI



PAs: Direct instruction is a more appropriate term than supervision PAs are a dependent occupation and not on the pathway to autonomous practise that clinical supervision provides for doctors @bmj_latest @TheDA_UK @drmattuk @Anisocyte @ExplosiveEnema2 @medicalmodelbri @TYoungstein @mmamas1973 @doctor_oxford @DrSteveTaylor @DrLKVaughan @DrNeenaJha @RobLaurensonD4P @iDrSunny @Roddy_Neilson @Azeem_Majeed bmj.com/content/389/bm…