Sabitlenmiş Tweet
CQD🧭🪶
492 posts



Balloon day 🎈
And my birthday happens to also be the day the Belkan War starts in Ace Combat Zero.


English


I actually presented this patient a few years ago as an educational case at SHM 2023 so you guys can take a look at the slides! Even if you have zero training with ultrasound, you can tell that the right eye has something going on! That jiggly bit isn't supposed to be there!
GIF
English
Retinal detachment is pretty nutty to encounter as an internal medicine doctor seeing a patient in the ED, but it definitely highlights the importance of taking a good history and having the proper exam skills, and not just taking the emergency team's evaluation for granted. 🗒️
This was really one of those cases where if I hadn't had the exact same presentation and sequence of events one time back in residency, I might have missed this diagnosis entirely! I could've admitted the patient as a stroke workup per the teleneurologist and emergency doc, and wasted critical hours in getting them the ophthalmological help that they needed.
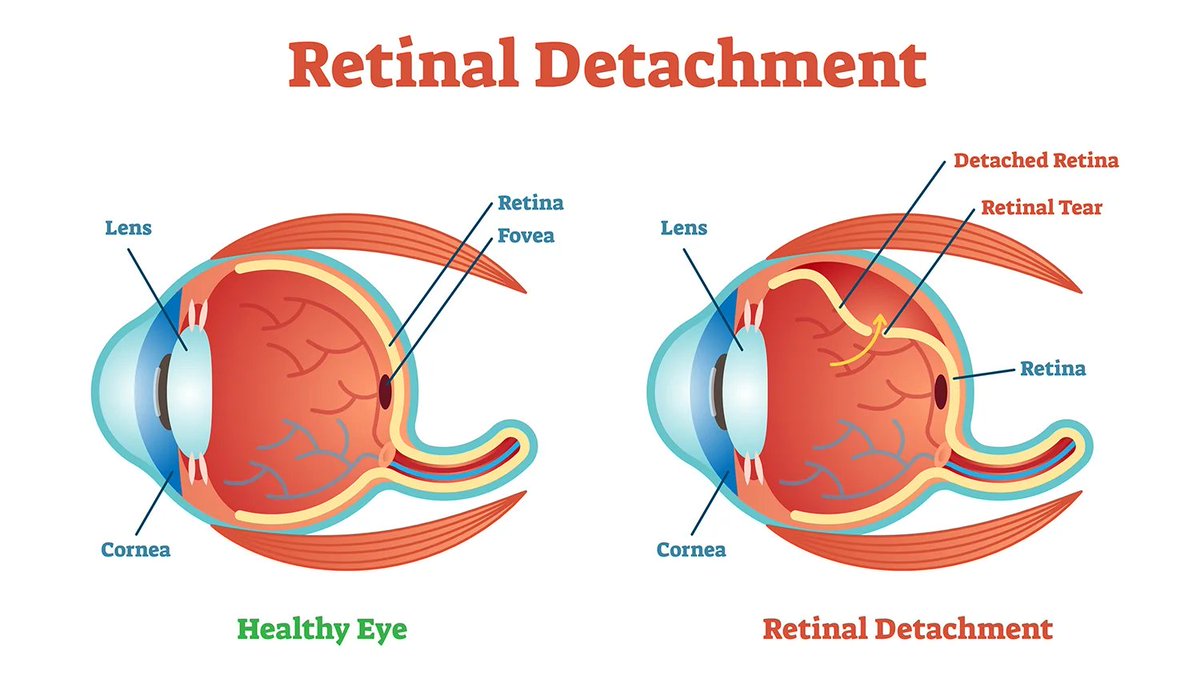
So retinal detachment in itself is not too common of a diagnosis, and usually happens spontaneously either in cases of facial trauma, or in the eldery. It can also happen as a consequence of late-stage diabetic retinopathy or in a patient with Marfan's (a genetic connective tissue disorder). Due to its namesake pathology, the retina will pop off the retinal pigment epithelium, causing monocular vision loss. But sometimes this can be unclear for the patient to describe or the provider to evaluate, prompting a stroke workup for a neurological issue, instead of a physical, eyeball issue.
Retinal detachment isn't going to show up on a CT or MRI as part of a stroke workup. So if you're not an eye doctor or an expert with the ophthalmoscope, the absolute quickest way to see if retinal detachment is the problem or not is to do an ocular ultrasound. Like seriously, just slap a tegaderm on the patient's eye, squeeze your gel, and start using the probe. Basically you get the patient to look around and try to blink behind their eyeball, and if the retina is detached, you can clearly see the floating layer bounce around. It is actually extremely easy and quick to perform, and I think more people should be familiar with doing this on ultrasound, since you can really save someone's eyesight with a 2 minute exam.
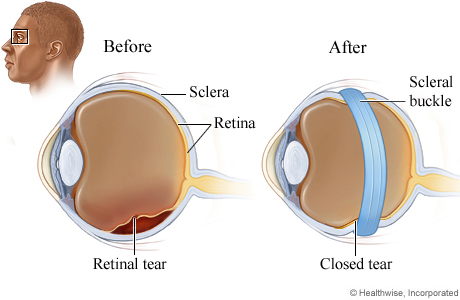
It's important to remember that RETINAL DETACHMENT IS A SURGICAL EMERGENCY, so early diagnosis by the provider is key. And unless you're presenting to an ED that's stocked with an ophthalmologist on consult (which is neither of the hospitals where I had these patients) that means it is going to be on the EM and IM providers to get it right. Ultimately, for both of these cases, I caught them both in the ED and could initiate early transfer to a hospital for surgery for scleral buckling. Waiting until the morning after to do the workup, or for the MRI to come back negative to prompt an eyeball investigation may have been too late to save their eyesight!
(hopefully this patient got scleral buckling done too, apparently there's another procedure for superior retinal detachments called pneumatic retinopexy where they inject sulfur hexafluoride or perfluoropropane gas straight into the vitreous body and the pressure differential just seals the retina back up against the epithelium and whoaaaaaaaa thats kinda gnarly)


saiken, M.D. 💜🩺 doctor irl & vtuber@saikenMD
Keep up with your ultrasound skills because 1 - it will save your patients 2 - it will save your license
English


I just finished one of these last night, right out of the gold tin pan. You simply don't eat it any other way.
Lauren 🩲@lllaurenA
The foreign part is eating it on a plate. Canadian law states it must be consumed straight from the pan.
English