Sabitlenmiş Tweet

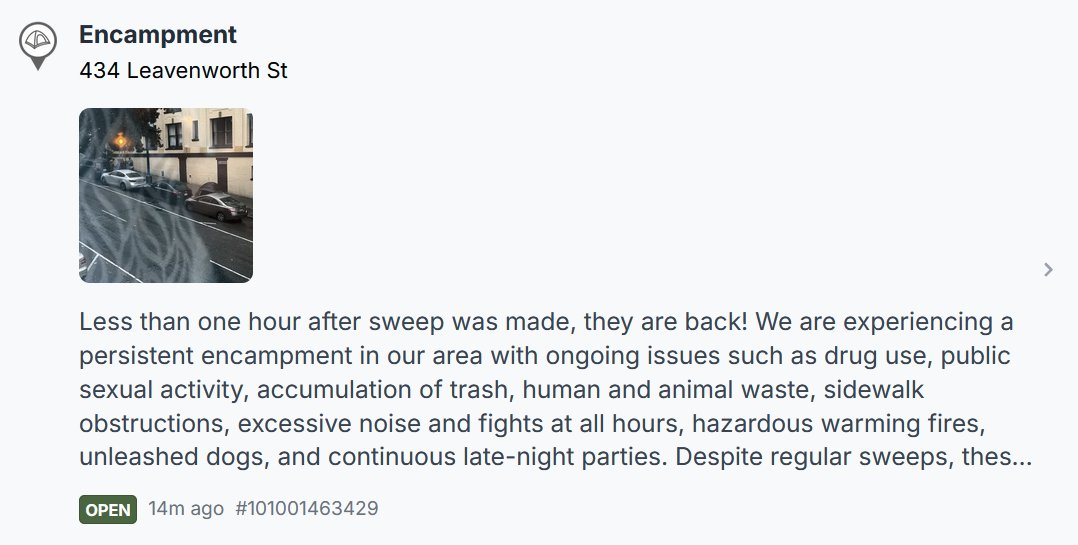
Why is there no means for reporting Vehicular Encampments via @SF311?
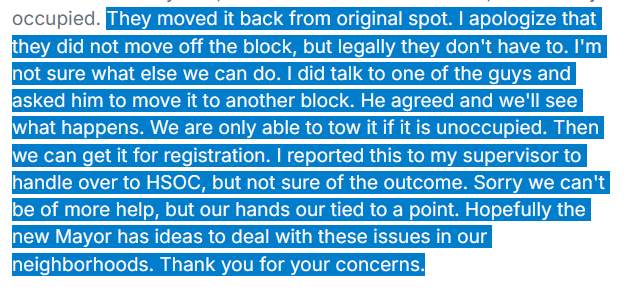
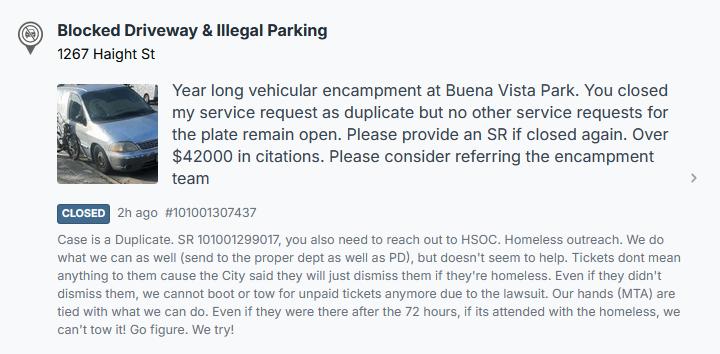
This recent response from MTA parking officials, regarding a yearlong encampment in front of a tent fire site at Buena Vista Park, reflects the current state of inter-dept cooperation at @sfgov. @kunalmodi
"Case Closed" SF311@CaseClosedSF311
A tale of two apps (San Jose 311 vs. San Francisco 311).
English