Sabitlenmiş Tweet

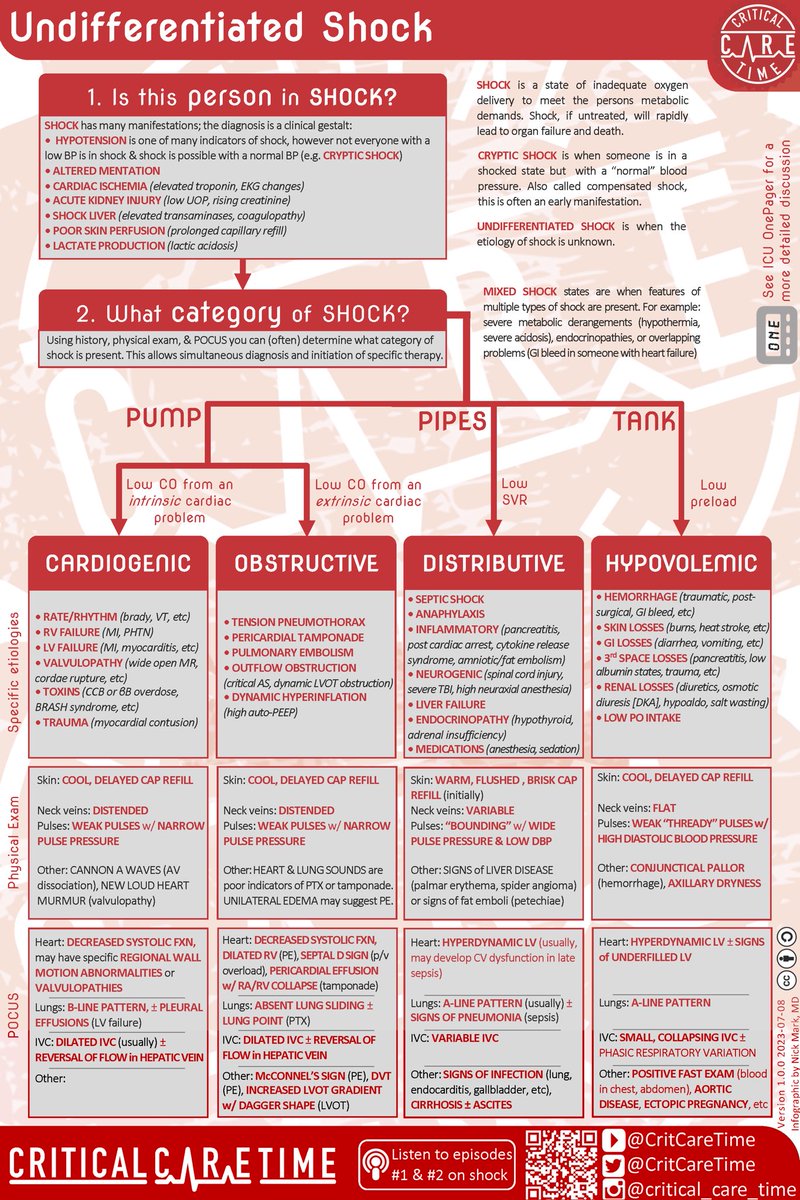
Check out our 🆕 infographic on undifferentiated shock; the perfect accompaniment to the first episode of Critical Care Time!
Part 1️⃣ shows.acast.com/649181182c969b…
Part 2️⃣ shows.acast.com/649181182c969b…
English
Critical Care Time
501 posts

@CritCareTime
The podcast for everyone who cares for the critically ill






Ketamine-Only Intubation in DKA: No paralytic = No apnea Preserves CO2 blow-off Sedation without respiratory arrest Key: Nebulize lidocaine first to numb the airway & prevent vomiting. Watch the cords move as you tube! Comment to discuss.