
Deepu Sethi
2.3K posts

Deepu Sethi
@DeepuSethi
Consultant Orthopaedic Knee Surgeon. Former Racing Driver & father of twins.
London, England Katılım Mart 2010
907 Takip Edilen1.3K Takipçiler




Deepu Sethi retweetledi



Ortho residents and sports fellows. This is a classic image.
Why does this person have exquisite medial pain.
English
@sayanamk I would certainly discuss fixation with patient. Young active patient, surgery may reduce (but not stop) future degenerative change. Balance with rehab and risks #informedconsent
English

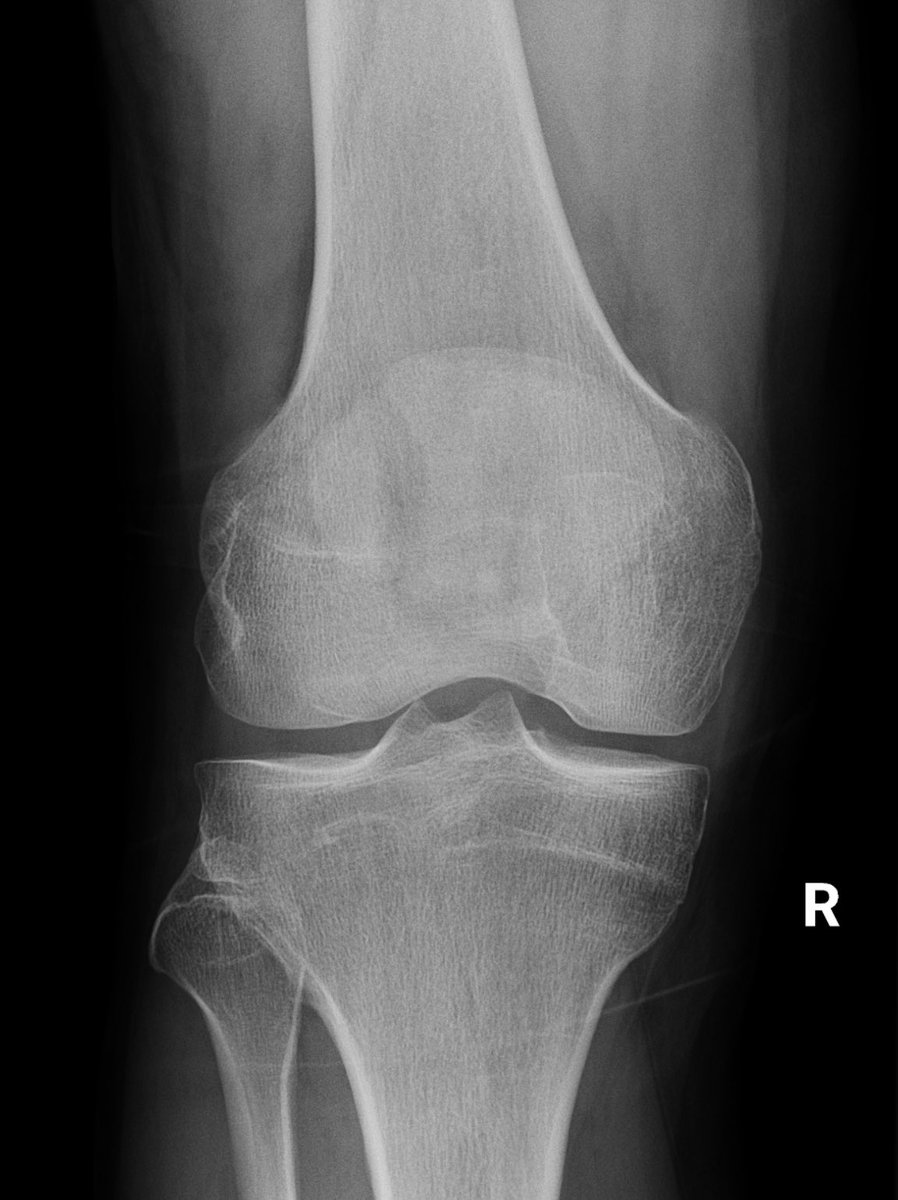
10 week old injury in a 40-year old, biker
Normal gait, able to straight leg raise, knee flexion 0° - 130° , Clarke’s test positive
#Orthotwitter - would you fix it or leave it ?

English
Deepu Sethi retweetledi

Attention knee surgery trainees!
A last minute change has meant we have a knee fellowship post available starting August 2024. One year post (or 2 x six months)
Come join the team of 8 specialist knee consultants to improve your knowledge of sports knee and arthroplasty
English
Certainly something to note in all ACL tears. In a primary with a high slope it is useful to counsel the patient explain that they may have a higher risk of re-injury. But slope correction in a primary, no. May add a LET to reduce risk of reinjury.
RJ@northwoods1980
Has anyone studied or currently studying for primary reconstruction?
English

@miriam_khalil13 It’s just never going to be as elegant as Orthopaedics I’m afraid 😉
English


@DrJN_SportsMed Great description of these chronic tears. We are understanding more about them and in some, surgical repair is very helpful
English
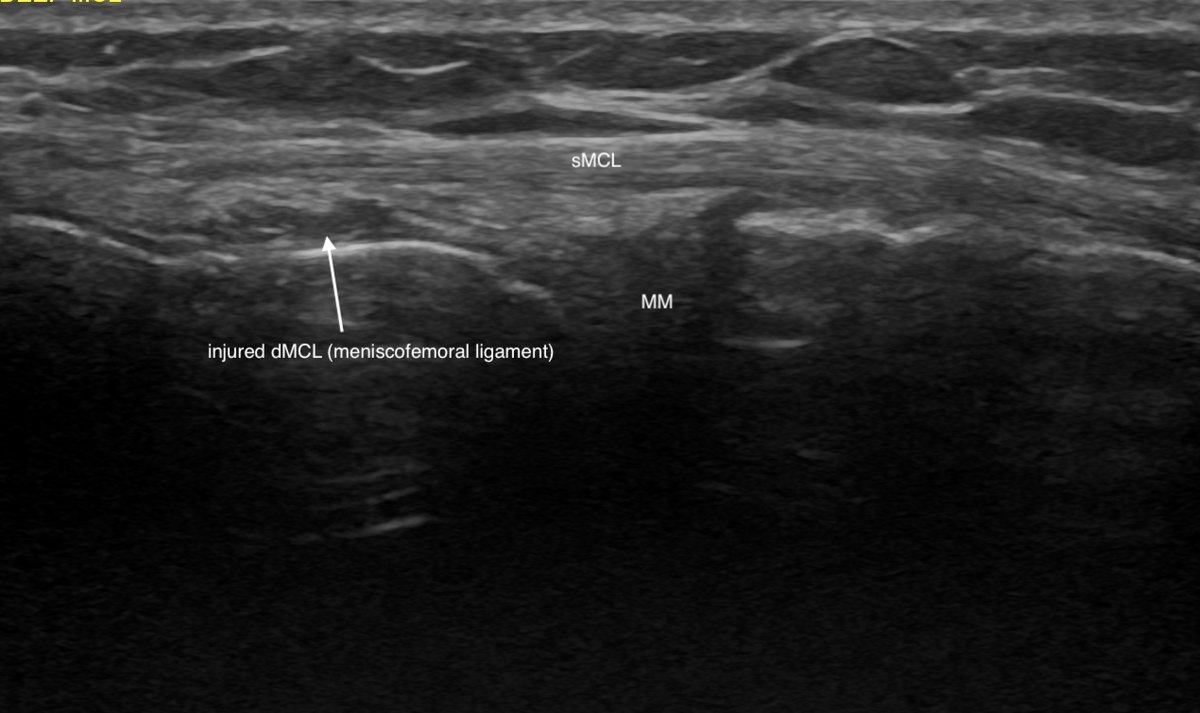
Consent ✅
Caught edge of ski moving slowly on ice 1 year ago - abrupt valgus / external rotation
Immediate medial knee pain, but settled quite quickly
No effusion
Since, nagging medial aching particularly on rotational movement eg side pass football, pivoting in tennis (can be sudden / sharp) - lost confidence in knee
Pure lateral movements - side step - ok
Exam - some subtle increased travel on anteromedial glide. No overt valgus laxity vs contralateral side
Tender on firm palpation proximal MCL
POCUS - chronic 'sprain' (arrow) of deep MCL (meniscofemoral ligament) - superficial MCL intact, meniscus normal
These deep MCL injuries can niggle on for ages, the key symptom is rotational provocation
English

13 years ago, Mrs MSK Radiologist welcomed me into her family…..
What a privilege to have been so included.
#HinduWeddings
#Verona
#orthotwitter

English
@DrJN_SportsMed I agree with @bellkneesurgeon and @kashakhtar MRI is a static image and aids in diagnosis. Management is decided by basics of history and examination. If persistent instability after adequate rehab, the “healed” ACL is clearly not functional.
English
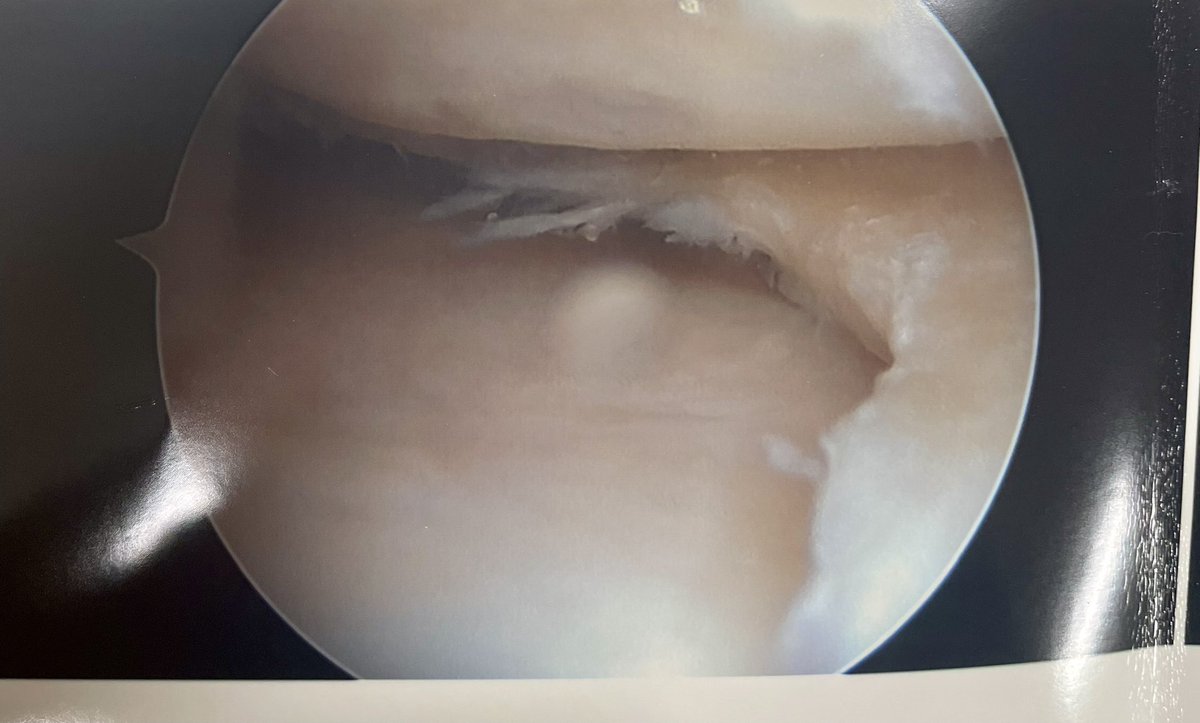
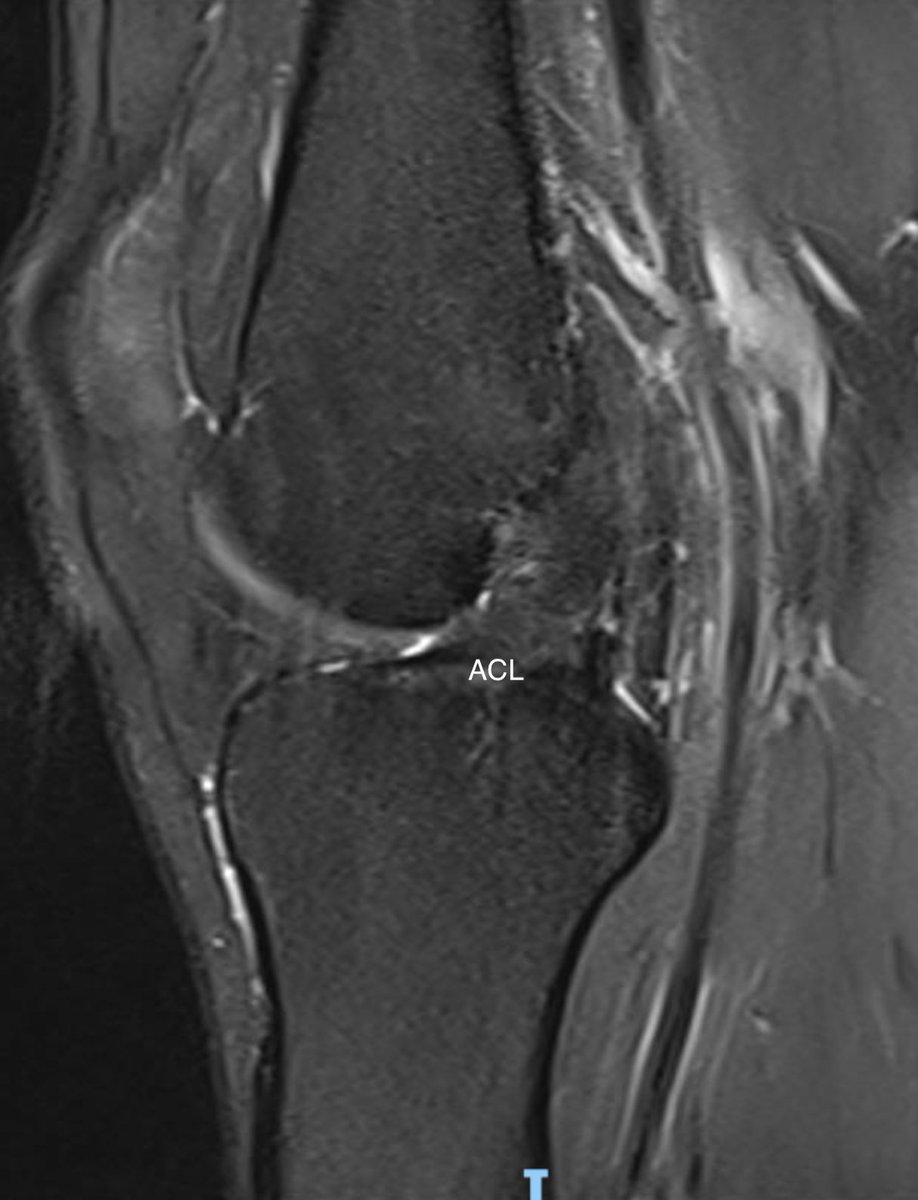
Consent ✅
Relevant case with respect to the 'healing' ACL & conservative management of ACL rupture debate
Footballer, twist, 'pop' & rapid onset swelling 2 years ago
Returned to football but struggled with sensation of imminent giving way / instability esp on change of direction
Few buckling episodes
Exam - increased travel on Lachman's testing, but firm-ish end point
MRI - healed ACL (thickened / scarred / in continuity)
So radiological healing definitely occurs, but doesn't necessarily tally with functional recovery

English
@kashakhtar @expertknee Needs de-rotation - not just coronal correction
English

@expertknee Surely you must have been seriously considering a double level osteotomy!
English


Deepu Sethi retweetledi

We have started randomising participants for METEOR2!!
👏👏👏 to everyone working on this super-important knee RCT
Do you see patients with persistent pain >6m after meniscectomy? Send them to one of the trial sites!
(sites & more details in thread..)
GIF
English

ACL Friday!
ACL reconstruction is tailored to the individual patient. In this example this is an 8 mm diameter graft in a small patient with a narrow notch. Note the position of the graft in the notch as the knee goes thru motion. A larger graft would potentially overstuff it.
English
English
@baskonline are delighted to announce a soft tissue knee cadaveric training day in conjunction with @ArthrexUK at their amazing facility in Solihull in April. We have 16 places, to be chosen from TPD nominations.
(instagram.com/p/C3iWzdGIRSQ/… for awesome music)
#bestofthebest

English
@DrJN_SportsMed @kashakhtar Yes, cysts around proximal tib-fib joint are quite common. Can cause pain, but often incidental finding.
English
Consent ✅
The proximal tibiofibular joint is an under-estimated source of lateral knee pain
Ganglion cysts arising from the joint can be a giveaway on imaging 🚨
It can be quite challenging to inject US guided as a 'tight' joint esp if degenerative 😤
Injection 'hack' - use the cyst as a portal to the joint - much easier target🚪
Video shows injection of cyst (anechoic black structure)
Needle comes from R side of screen - filling up, retrograde flow into joint
English
Français

@DeepuSethi @KneeUnit @kneedoclond @kashakhtar @expertknee Living donor quad tendon allograft for ACL would be a worthy cause and treatment.
English
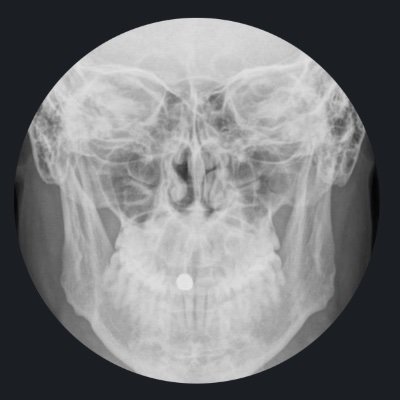
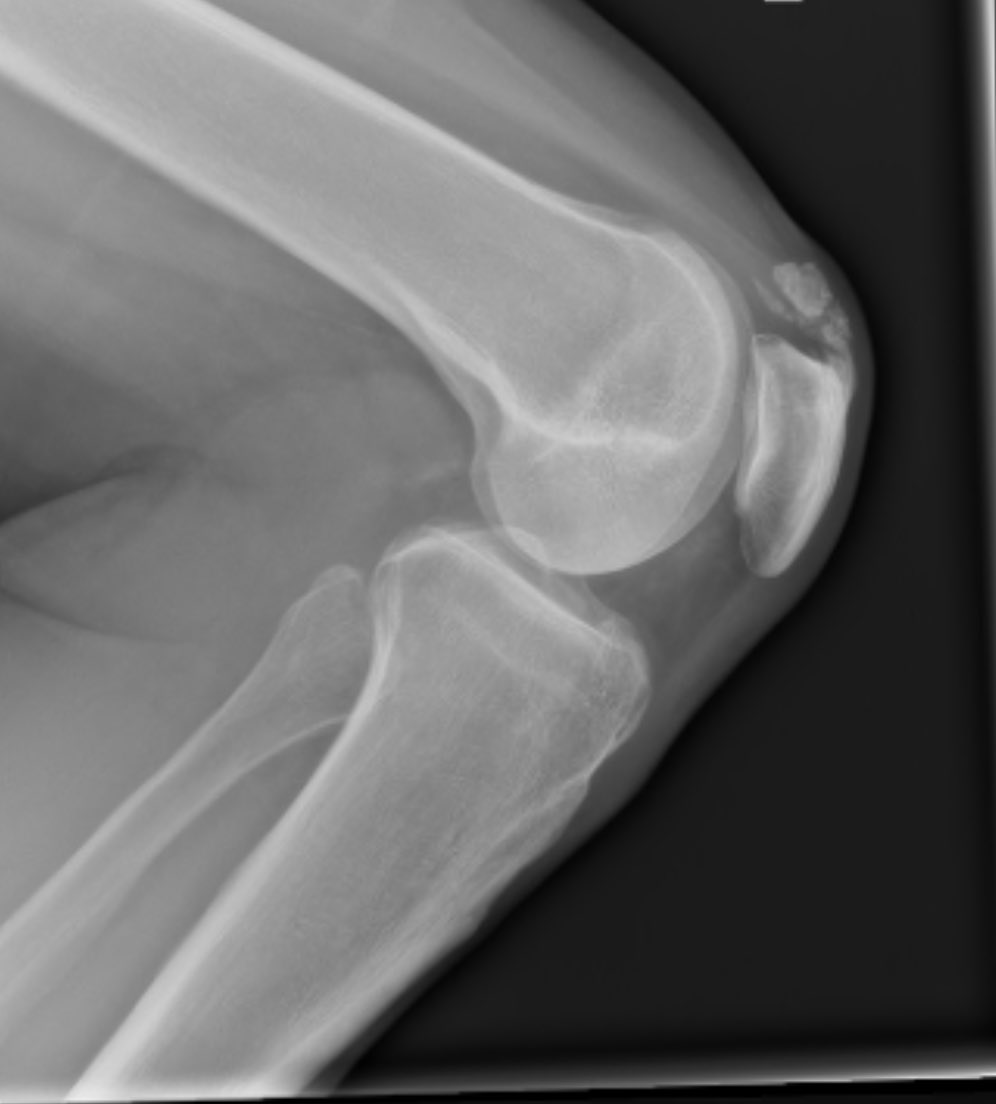
Interesting case. Calcific tendonitis in distal quadriceps. Symptomatic, treatment options? @KneeUnit @kneedoclond @kashakhtar @expertknee
English
@DrJN_SportsMed @kashakhtar @expertknee @KneeUnit @kneedoclond Yes, not seen one this amount of calcification before - admittedly I don’t use ultrasound, but I do see a lot of knee x-rays
English
@kashakhtar @expertknee @DeepuSethi @KneeUnit @kneedoclond Agree these are quite big deposits though…
English
English
@DeepuSethi @kashakhtar @expertknee @KneeUnit @kneedoclond I’d assess distal soft tissue & deposits first on US - then consider SWT, deep quad tendon CSI or barbotage depending on what feel i get for it. Then rehab with experienced knee physio.
any history gout?
English
@kashakhtar @expertknee @KneeUnit @kneedoclond @DrJN_SportsMed Thinking this is quite a big lesion and very well calcified. Speaking to shoulder surgeons, they use shockwave and needling, but for much smaller lesions.
English
@expertknee @DeepuSethi @KneeUnit @kneedoclond Likewise. Have taken some Osgood Schlatter's ossicles out of inflamed distal patella tendons, but rare to see calcific tendonitis.
Didn't SEM use to shockwave these @DrJN_SportsMed ??
English