@propofoldream @MichiIntrona We have one going through ethics at the moment. Main limitation for generalisability will be it's only designed to investigate this in adolescents, so a similar one in adult land would be most helpful...
English
Dr Matt Hart
309 posts
@DocMattHart
Paediatric Anaesthetist. Regionalist and TIVA diva.


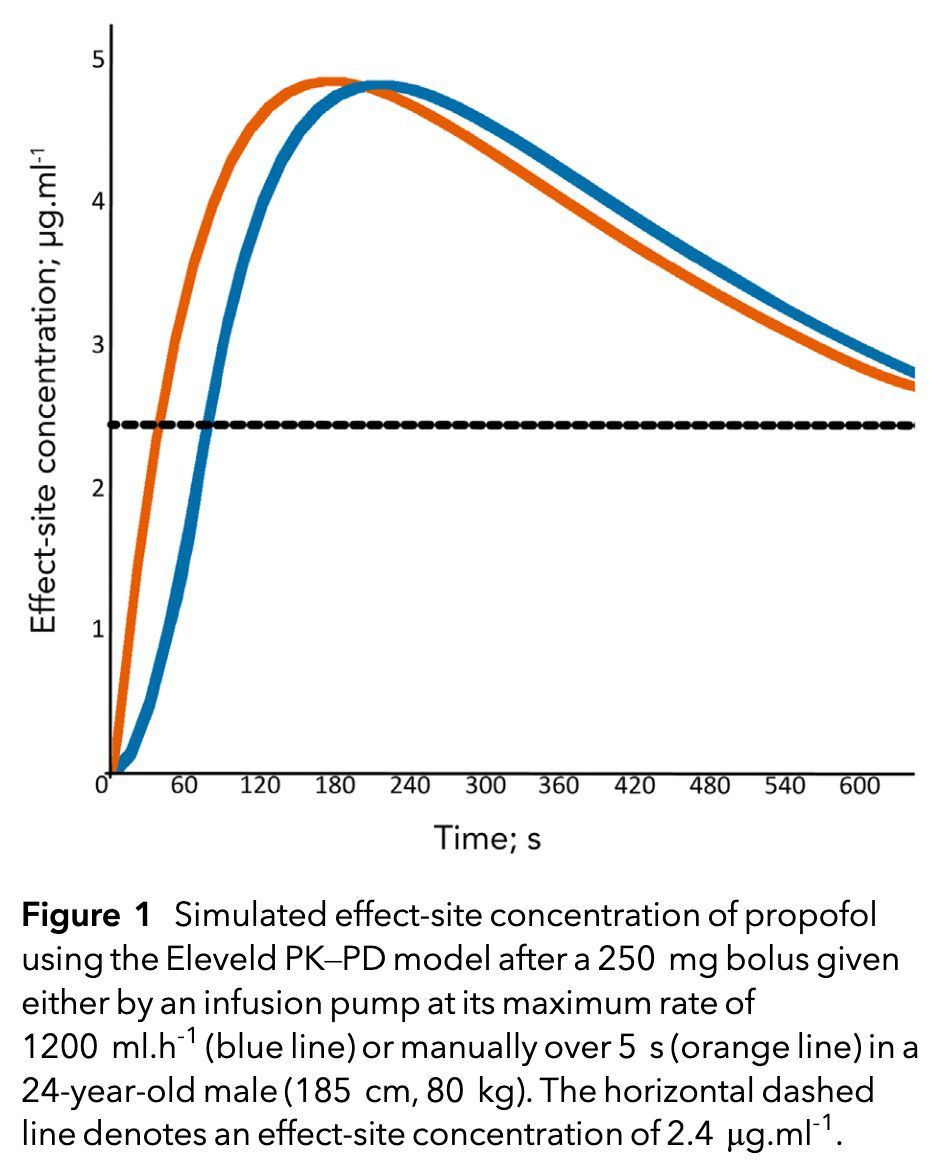
A few things: Manual bolus is over 15secs. I reckon I’d typically deliver the initial bolus over ~3 secs. Time to peak effect is not what’s relevant, it’s time to sleep. Clinically this is not the case. TCI inductions (even for non-RSI) are much slower (too slow) inductions.

Target-controlled infusions have been criticised as too slow for RSI, due primarily to the maximum infusion rate of most pumps (~1200 ml/h). Effect-site concentrations at time-to-peak effect were nearly identical between target-controlled and manual infusions. #anaesthesia #MedTwitter doi.org/10.1111/anae.7…
The chance of having an allergic reaction to a neuromuscular blocking drug is: • suxamethonium: ~1 in 1500 people • rocuronium: ~1 in 3300 people • atracurium: ~1 in 15,000 people Women were up to eight times more likely to have a reaction than men. #anaesthesia #MedTwitter #allergy doi.org/10.1111/anae.7…