Prashant chotalia retweetledi

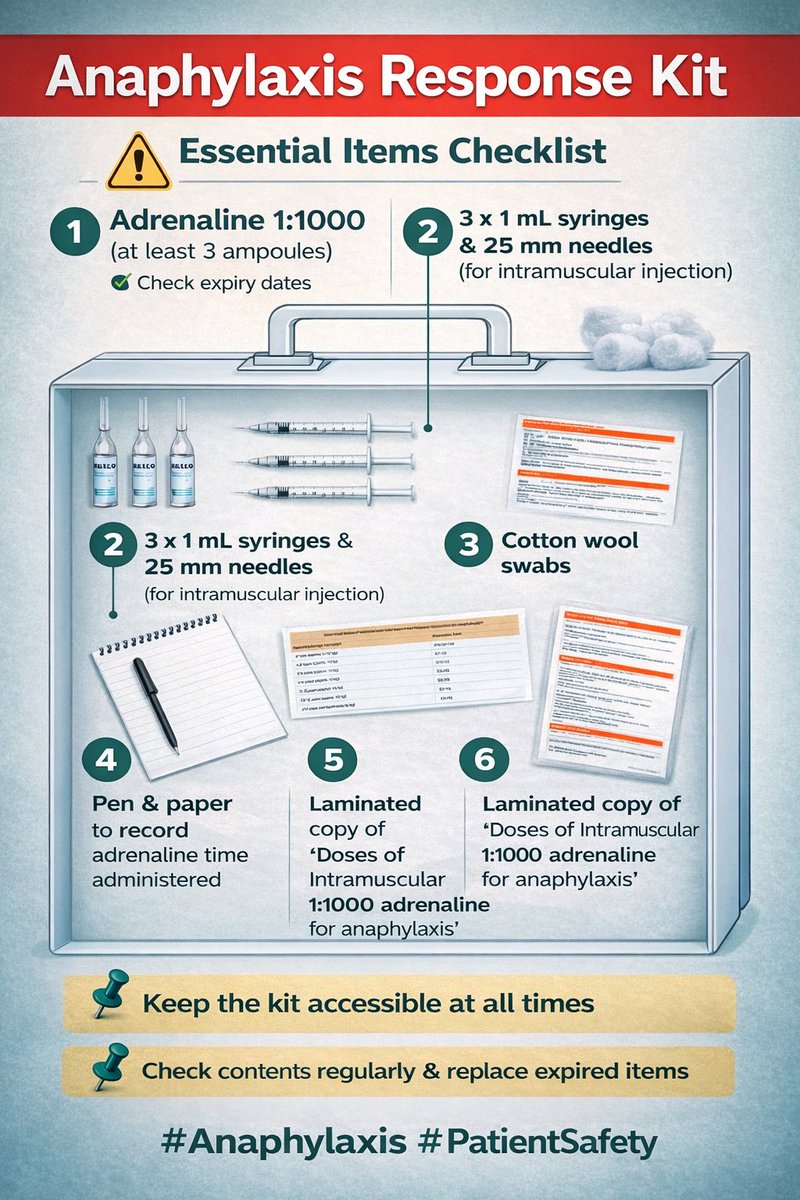
🧰 Anaphylaxis Response Kit — be ready before it matters.
Every clinical area should have an accessible kit with IM adrenaline 1:1000, syringes, dosing charts, and clear guidance.
Regular checks save lives.
Early adrenaline. Right dose. Right time.
#Anaphylaxis #AllergyCare #EmergencyMedicine #PatientSafety #MedEd #Healthcare #Adrenaline #ClinicalSafety #SaveLives
English