Andreas Müssigbrodt retweetledi

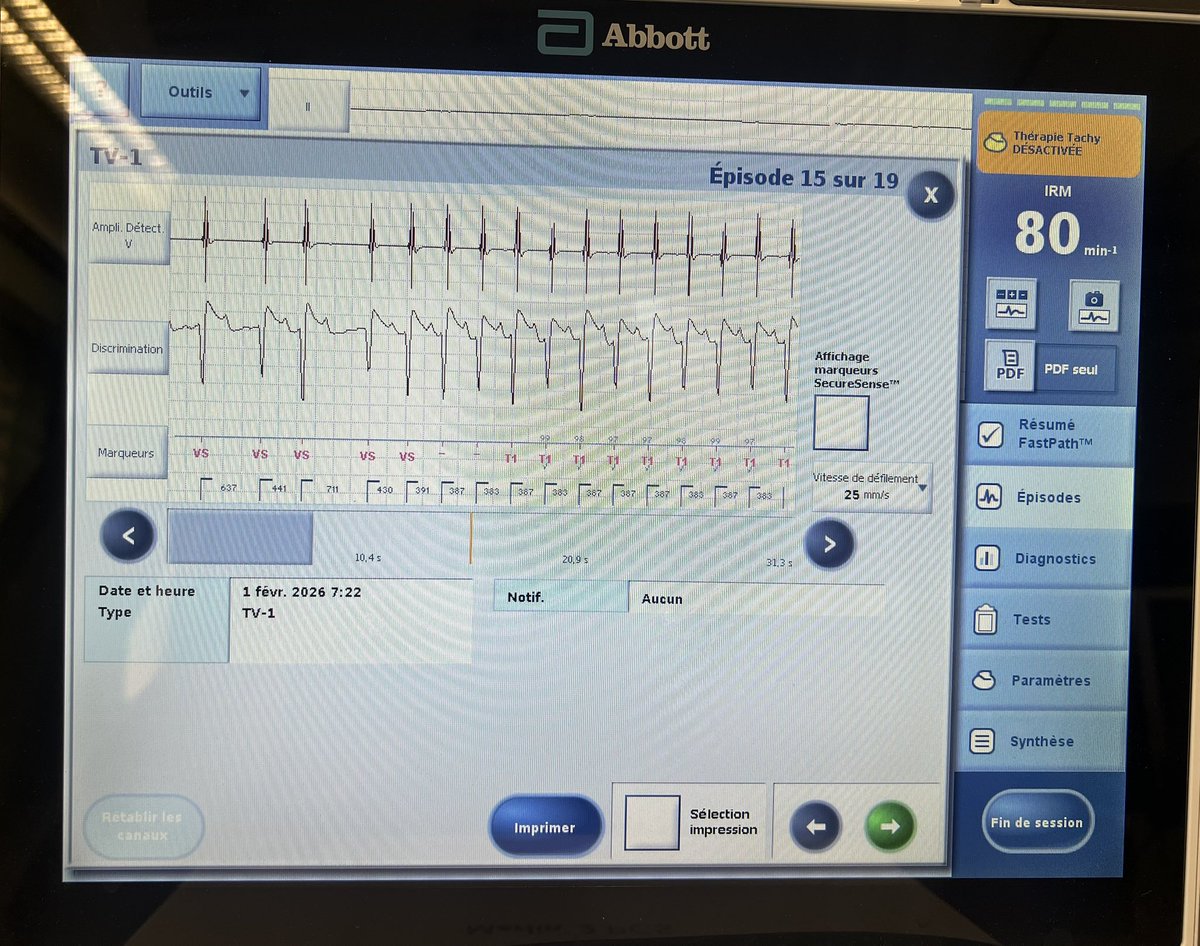
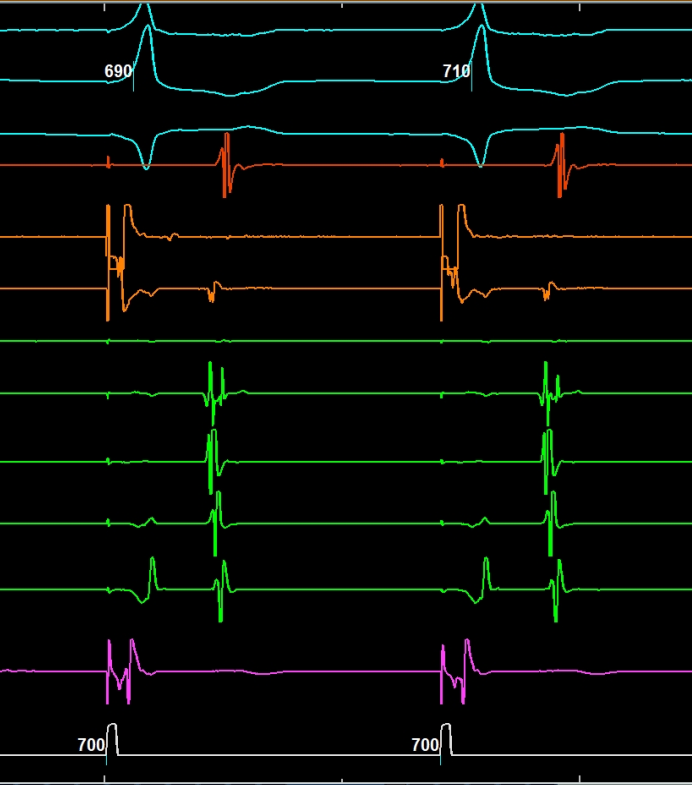
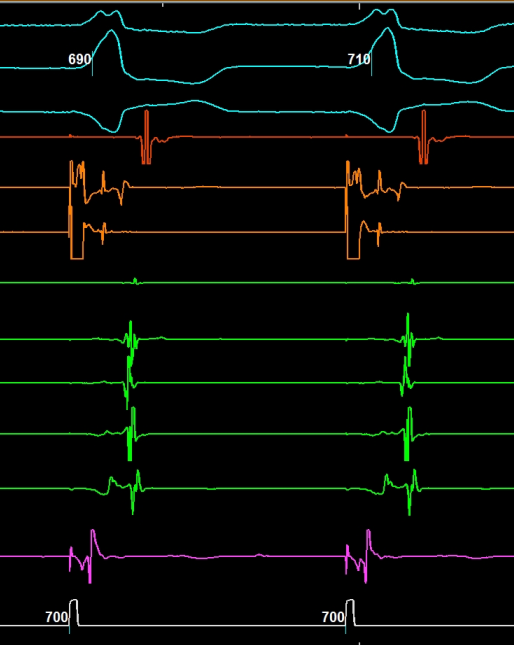
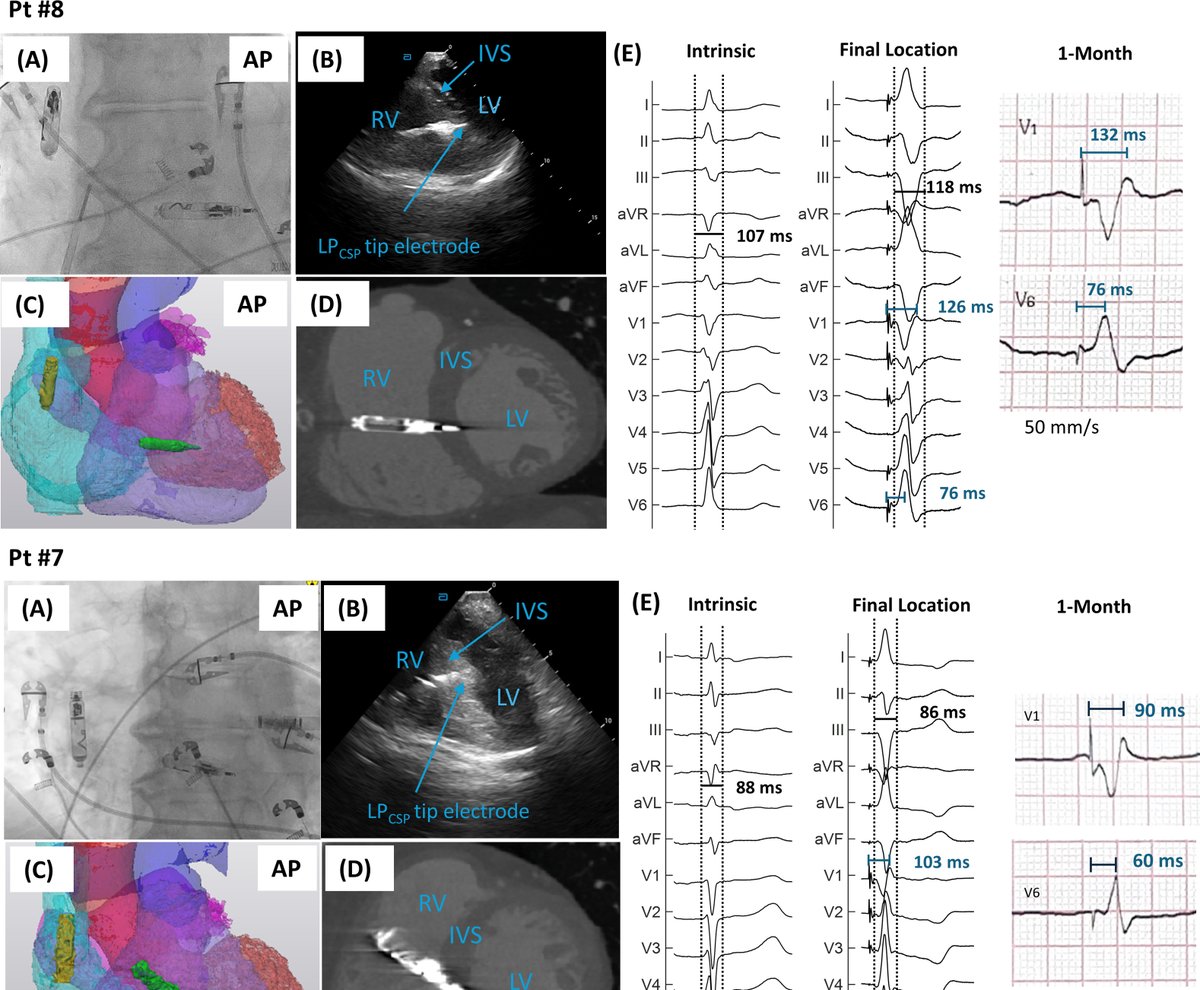
LEAP2: A First-in-Human Evaluation of a Chronically-Implanted Novel Leadless Pacemaker for Conduction System Pacing #OpenAccess
heartrhythmjournal.com/article/S1547-…
English
Andreas Müssigbrodt
2.2K posts
@EPWaveDoc
Associate Professor, FESC, FEHRA, Cardiac Electrophysiologist, Sports Cardiologist, Editorial board JICE, Surfer and Kitesurfer 🏄🏽♂️, Sarcoma Survivor












#SportsEP is having a moment, and we're all in! Kicking off #HRS2026 in Chicago, Global Summit 2026 will bring together international leaders to tackle one of the biggest topics in EP today. Dive into fascinating conversations on: 🏈 Arrhythmias in Athletes 🏀 Exercise & Cardiovascular Health ⚽ Physiological Monitoring & Safety ⚾ SCA Prevention Join the huddle and RSVP: bit.ly/3O6bB2p Not registered for the meeting yet? Get in the game: bit.ly/3KzGmLs @EduardoSaad3 @eugenechung01 @bdebneygray @SusanEtheridg12 @PrashSanders



In high-risk atrial fibrillation with cerebral amyloid angiopathy, anticoagulation was associated with lower ischemic stroke and mortality without increased risk of intracranial hemorrhage or major bleeding. By @HAlvinChenNeuro link.springer.com/article/10.100…





A first look at this year’s London Arrhythmia Summit programme ✔️ Guideline updates ✔️ Keynote session ✔️ Device therapy & pacing debates ✔️ AF ablation challenges ✔️ AI in arrhythmia ✔️ VT strategies londonarrhythmiasummit.com
Impact of Left Atrial Posterior Wall Isolation using Pulsed-field Ablation in Patients Undergoing Repeat Catheter Ablation for Atrial Fibrillation #OpenAccess heartrhythmjournal.com/article/S1547-…