Jonathan Hindmarsh retweetledi
Jonathan Hindmarsh
485 posts


Jonathan Hindmarsh
@Hindmarsh_Jon
Pharmacist in Palliative Care MRPharmS (Consultant). Independent prescriber. Advanced Clinical Skills. @sunderlandroyal @stbenedicts1984
Sunderland, England Katılım Mayıs 2017
220 Takip Edilen274 Takipçiler
Jonathan Hindmarsh retweetledi
Jonathan Hindmarsh retweetledi
Jonathan Hindmarsh retweetledi

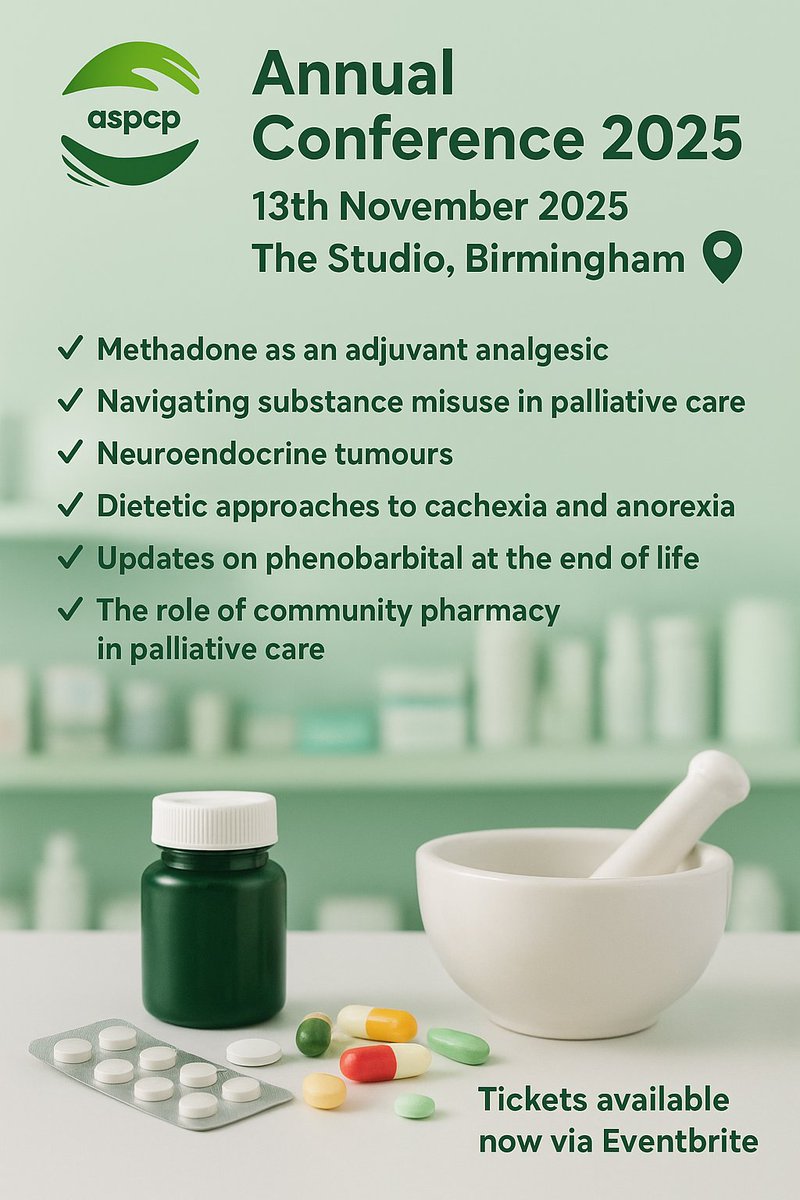
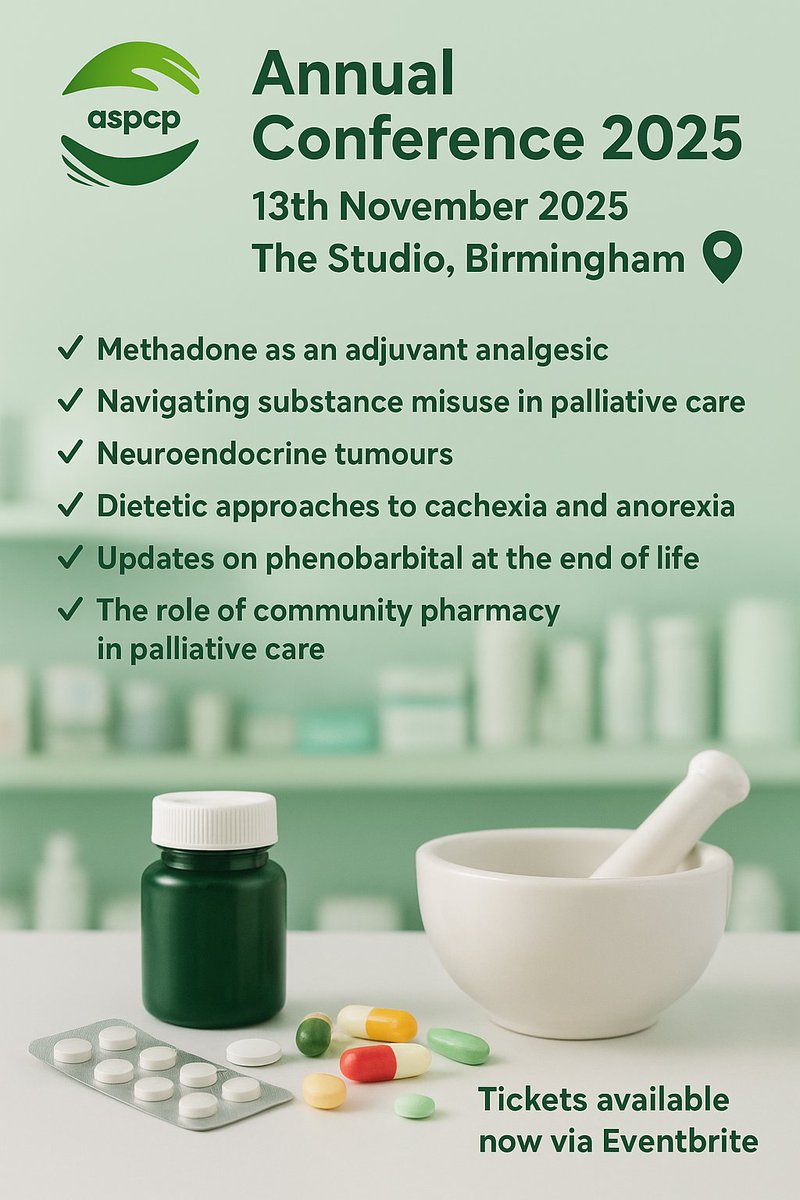
ASPCP Annual Conference 2025
Join us on 13 Nov, Birmingham for a full day of expert-led learning in palliative and EoL care.
🎯 Topics: Symptom control, prescribing, MDT collaboration
🤝 Network with peers & stay ahead of best practice share.google/FcfMXjaPRULEd4…
English
Jonathan Hindmarsh retweetledi
💊Venlafaxine and blood pressure💊
A dose-dependent link between venlafaxine and elevations in blood pressure has been suggested by some studies. Additionally, case reports have implicated venlafaxine as the precipitating cause for hypertensive crisis in some individuals.
English
Jonathan Hindmarsh retweetledi
Jonathan Hindmarsh retweetledi
Exciting news! Due to pharma funding, ASPCP conference tickets are now just £30. 🎉 Open to everyone—members and non-members! A great opportunity to connect, network, and hear from top speakers. We appreciate your continued support! #ASPCP #PalliativeCare #Conference
eventbrite.co.uk/e/aspcp-annual…
English
Jonathan Hindmarsh retweetledi

#Pharmacy - share your opinions, examples of service delivery & best practice on #palliative and end-of-life care.
We also want to hear what practical, educational materials you need.
More in @PJOnline_News' 'Call for papers' announcement ⬇️
The Pharmaceutical Journal@PJOnline_News
‘Call for papers’: palliative and end-of-life care #ThePJ would like to invite UK pharmacy professionals to let us know what they are doing in their local area to improve access to palliative and end-of-life care #callforpapers #palliativecare pharmaceutical-journal.com/article/opinio…
English
Jonathan Hindmarsh retweetledi
Join us for the annual conference of the Association of Supportive and Palliative Care Pharmacy, where you'll gain valuable insights and network with fellow palliative care experts.
14th November 2024 at The Studio, 7 Cannon St, Birmingham.
eventbrite.co.uk/e/aspcp-annual…
English
Jonathan Hindmarsh retweetledi
Book now 👇
eventbrite.co.uk/e/aspcp-annual…

ASPCP@theASPCP
Join us for the annual conference of the Association of Supportive and Palliative Care Pharmacy, where you'll gain valuable insights and network with fellow palliative care experts. 14th November 2024 at The Studio, 7 Cannon St, Birmingham. eventbrite.co.uk/e/aspcp-annual…
English
Jonathan Hindmarsh retweetledi

Jonathan Hindmarsh retweetledi
💊Opioids + immunosuppression💊
Some opioids (especially morphine, methadone, and fentanyl) are immunosuppressive, reducing natural killer cell activity and neutrophil chemotaxis.
Four epidemiologic studies link prescription opioids to an increased risk of serious infections.
Case-control study: Opioid users had a 38% higher risk for community-acquired pneumonia (OR 1.38, 95% CI 1.08-1.76); highest for long-acting opioids (OR 3.43, 95% CI 1.44-8.21).
Tennessee Medicaid study: Opioid users had a higher risk of invasive pneumococcal disease (aOR 1.62, 95% CI 1.36-1.92); strongest for long-acting/high-potency opioids.
Hospitalization rates for serious infection were lower for oxycodone, oxymorphone, or tramadol users vs. morphine, methadone, or fentanyl users (aIRR 0.78, 95% CI 0.66-0.91).
Studies suggest opioids may increase serious infection risk, particularly with morphine, methadone, and fentanyl.
More research needed to confirm findings and assess risk variations by patient characteristics and pathogens
English
Jonathan Hindmarsh retweetledi
Duloxetine for Chemotherapy induced peripheral neuropathy (CIPN):
➡️ Initially proven effective in a double-blind trial with 231 patients.
➡️ Participants had painful CIPN, with pain scores >4/10 persisting for 3+ months.
➡️ Randomized to duloxetine (30 mg daily for 1 week, then 60 mg daily for 4 weeks) or placebo.
➡️ Pain scores measured weekly via Brief Pain Inventory, Short Form (BPI-SF).
➡️ Other endpoints: QOL assessed by FACT-GOG NTX and EORTC QLQ-C30, plus nonpainful symptoms.
➡️ After 5 weeks, a 2-week washout period occurred, followed by crossover to the alternate treatment.
➡️ Duloxetine group had a larger average decrease in pain score (1.06 vs. 0.34, p = 0.003).
➡️ Greater improvement in functional/QOL scores and reduced foot numbness/tingling (41% vs. 23%).
➡️ Well tolerated with no significant differences in toxicities.
➡️ More effective for oxaliplatin-induced than taxane-induced neuropathy.
Additional small trials:
➡️ One trial: venlafaxine, duloxetine, or placebo for CIPN; duloxetine showed more reduction in neuropathy.
➡️ Japanese trial: duloxetine outperformed vitamin B12 in 34 patients.
➡️ Phase II trial: duloxetine was inferior to pregabalin in 80 patients with taxane-related CIPN.
Guidelines:
2020 ASCO: clinicians may offer duloxetine for CIPN.
2020 ESMO/EONS/EANO: recommend duloxetine for neuropathic pain.
☀️ Benefit is modest but notable ☀️
English
Jonathan Hindmarsh retweetledi
💥💥 Naldemedine💥💥
Naldemedine is an amide derivative of naltrexone with structural modifications to limit its ability to cross the blood-brain barrier at therapeutic doses.
It acts as a peripherally-acting antagonist of opioid μ-receptors, used to treat opioid-induced constipation.
Administered orally as the tosilate, but doses are expressed in terms of the base; 260 mcg of naldemedine tosilate is equivalent to 200 mcg of naldemedine.
The usual dose is 200 mcg of naldemedine once daily.
Metabolized mainly by the CYP3A family; inhibitors or inducers of these enzymes may affect naldemedine concentration.
If potent or moderate CYP3A or P-gp inhibitors are used, monitor for naldemedine-related adverse effects.
Symptoms of opioid withdrawal and gastrointestinal disturbances reported during therapy, particularly at initiation.
Gastrointestinal perforation reported with similar drugs; manufacturer contraindicates use in patients with known or suspected gastrointestinal obstruction.
Stop therapy in patients who develop severe, persistent, or worsening abdominal pain.
Not recommended in patients with severe hepatic impairment due to lack of data.
English
Jonathan Hindmarsh retweetledi
💥💊Prucalopride💊💥
Prucalopride is a selective 5-HT4 receptor agonist used for chronic constipation when laxatives fail.
Standard dose: 2 mg once daily; elderly patients start at 1 mg once daily.
Efficacy not established beyond 3 months; reassess treatment regularly.
Not recommended for children; studies show no more effective than placebo.
Reduced dose (1 mg daily) in severe hepatic impairment (Child-Pugh class C).
Reduced dose (1 mg daily) in severe renal impairment.
Common side effects: headache, abdominal pain, nausea, diarrhoea, dizziness, decreased appetite, fatigue.
Use cautiously in patients with significant comorbidities, particularly ischemia heart disease, arrhythmias, intestinal perforation or obstruction, inflammatory bowel disease, or toxic megacolon.
Prucalopride does not affect cytochrome P450 but may be a weak substrate of P-glycoprotein; minor interaction with ketoconazole.
Rapidly absorbed from the GI tract, peak plasma in 2-3 hours, bioavailability >90%, low plasma-protein binding.
Excreted mainly unchanged via urine (60-65%) and faeces (5%); half-life ~1 day.
English
Jonathan Hindmarsh retweetledi

Jonathan Hindmarsh, advanced clinical Pharmacist is now updating us on best practices for patients with Parkinson’s Disease as they approach the end of life

English
Jonathan Hindmarsh retweetledi

Jonathan Hindmarsh retweetledi
Psychosis in Parkinson’s Disease (PD) Patients:
Psychosis can significantly impact a patient’s quality of life and overall well-being.
1. Assessment and Underlying Causes:
➡️Assess for potential precipitants or underlying causes of psychosis in PD patients.
➡️Consider factors such as infection, delirium, dementia, and adverse effects of anti-PD drugs or other medications.
2. Non-Pharmacological Strategies:
➡️Start with non-pharmacological approaches to manage psychosis:
➡️Address infections if found.
➡️Manage delirium or dementia if present.
➡️Monitor closely for changes.
3. Stepwise Pharmacological Management:
➡️If psychosis persists or worsens, consider pharmacological treatment options:
➡️Reduce or stop non-PD medications (especially sedatives, anxiolytics, and antidepressants).
➡️Balance the potency and likelihood of exacerbating psychotic symptoms when adjusting PD medications.
➡️Monitor patients closely during medication adjustments.
4. Antipsychotic Medications:
➡️Initiate antipsychotic therapy with specific agents:
➡️Pimavanserin, quetiapine, or clozapine (avoid other neuroleptics).
➡️Monitor patients for response and potential adverse effects.
4. Clozapine and Quetiapine:
➡️Clozapine and quetiapine are effective options for managing psychosis in PD.
➡️Remember to monitor patients closely throughout the management process, balancing symptom relief with potential side effects of medications.
English
Jonathan Hindmarsh retweetledi
Trimethoprim inhibits tubular creatinine secretion and can therefore cause a rise in serum creatinine levels without affecting true creatinine clearance, and may lead to a ‘false positive’ diagnosis of Acute Kidney Injury💊 🫘🩸
bmj.com/content/360/bm…
English