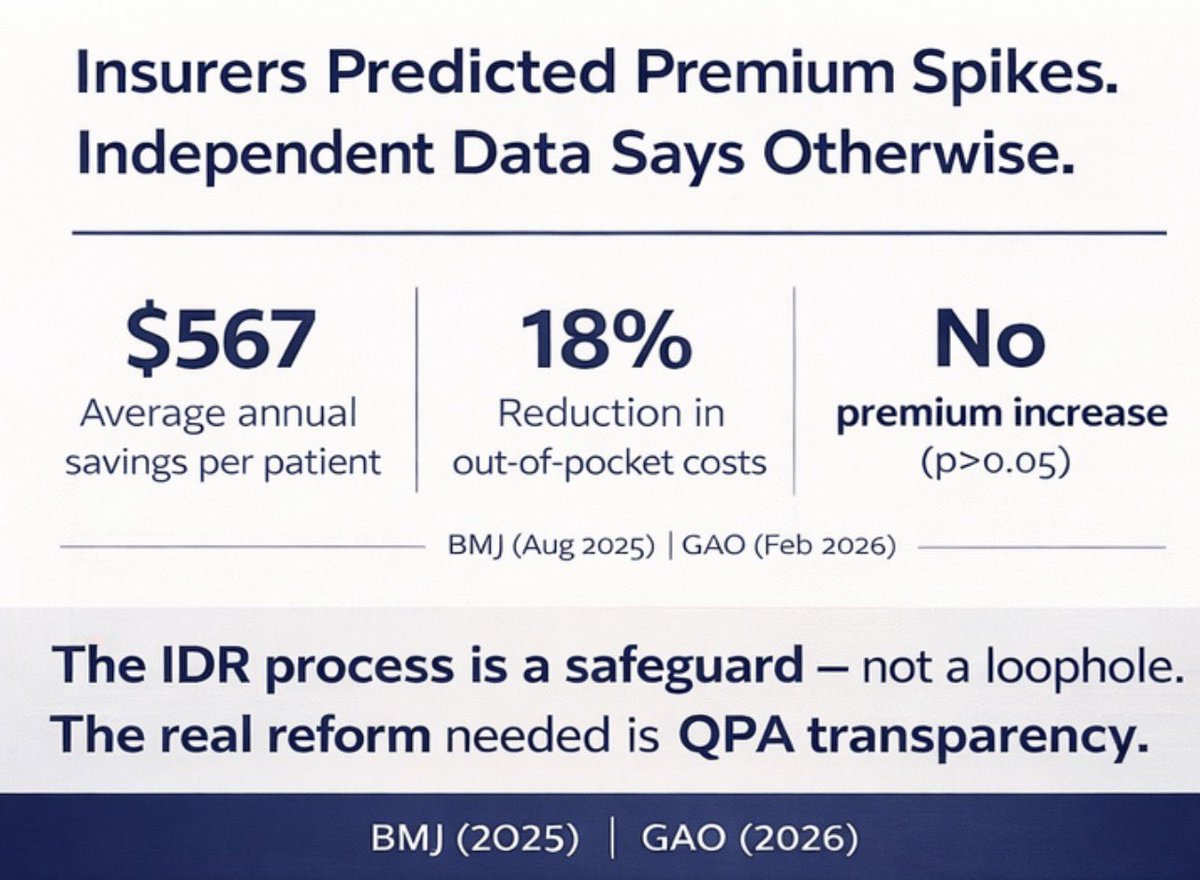
Two Major Studies. One Clear Conclusion: The NSA Works. Insurers agreed to the bipartisan No Surprises Act when it passed with overwhelming bipartisan support in 2020. Now those same insurers are lobbying to gut the law’s Independent Dispute Resolution process – the heart of the law that provides an independent body to determine fair payments. Two independent studies — one from Harvard-affiliated researchers published in The BMJ and one from the U.S. Government Accountability Office — arrive at the same conclusion, the NSA is working. ✅Patients in states newly protected by the NSA are saving an average of $567 per year in out-of-pocket costs, with no corresponding increase in premiums. ✅More than 10 million surprise bills were prevented in the first nine months of 2023 alone, and three of the four specialties most associated with surprise billing saw increased in-network participation after the law took effect. The insurers’ supposed cost-shifting never materialized. The market responded exactly as Congress intended – with more contracting, not less. The evidence is clear, and it's time to stop second-guessing whether this law works and start protecting it. 🔎 View the studies: indemed.org/wp-content/upl…