Sabitlenmiş Tweet
Irake
723 posts


Finishing off this week, we have Dr. Siegel giving an abdominal case review session on Sunday, May 24th, at 4 PM EST!
-Session style will be rapid-fire cases
Register here! us06web.zoom.us/meeting/regist…
English
Irake retweetledi
Finishing up this week strong, we have Dr. Agely giving an abdominal case review session specializing in biliary cases. It will be on Sunday, May 17th, at 4 PM EST.
-Style will be rapid-fire cases
Be there or be square! Register here! us06web.zoom.us/meeting/regist…
English

English
Irake retweetledi

Irake retweetledi

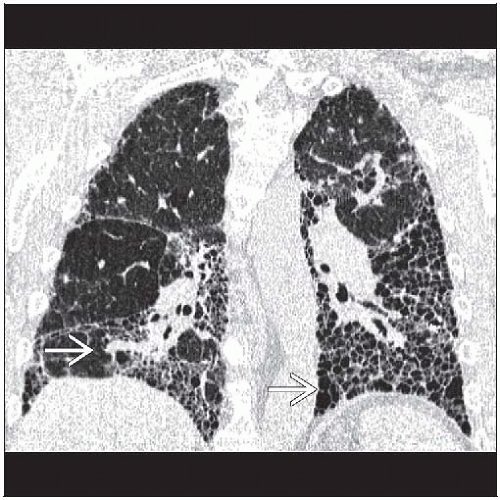
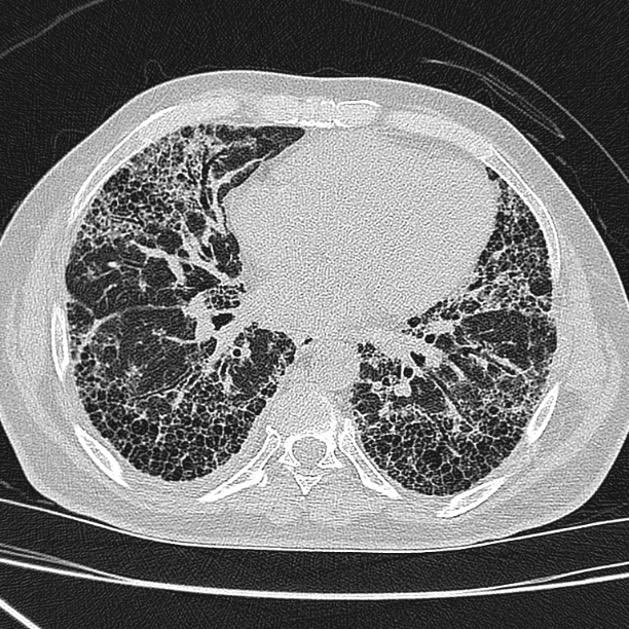
IPF is a diagnosis of exclusion in patients > 60 years old with "velcro-like" crackles 🩻
• Imaging (UIP Pattern): Look for honeycombing and peripheral, basal-predominant reticular opacities on HRCT
• The "Do Not Do" : Never give "Triple Therapy" (Prednisone, Azathioprine, N-acetylcysteine) for IPF; it was proven harmful in trials
Best Treatment options : Nintedanib or Pirfenidone (slows decline, doesn't reverse it though) & final option is Lung Transplant evaluation
English

Irake retweetledi

Irake retweetledi

Interventional Radiology Basics: The Micropuncture Set
youtu.be/axQmrW6iEyc Learn the first 3 steps of almost every endovascular procedure💉🩻! This set is high yield for any IR rotation #interventionalradiology #radiology #irad #futureradres #radres #iradres #meded

YouTube
English
Irake retweetledi
Irake retweetledi

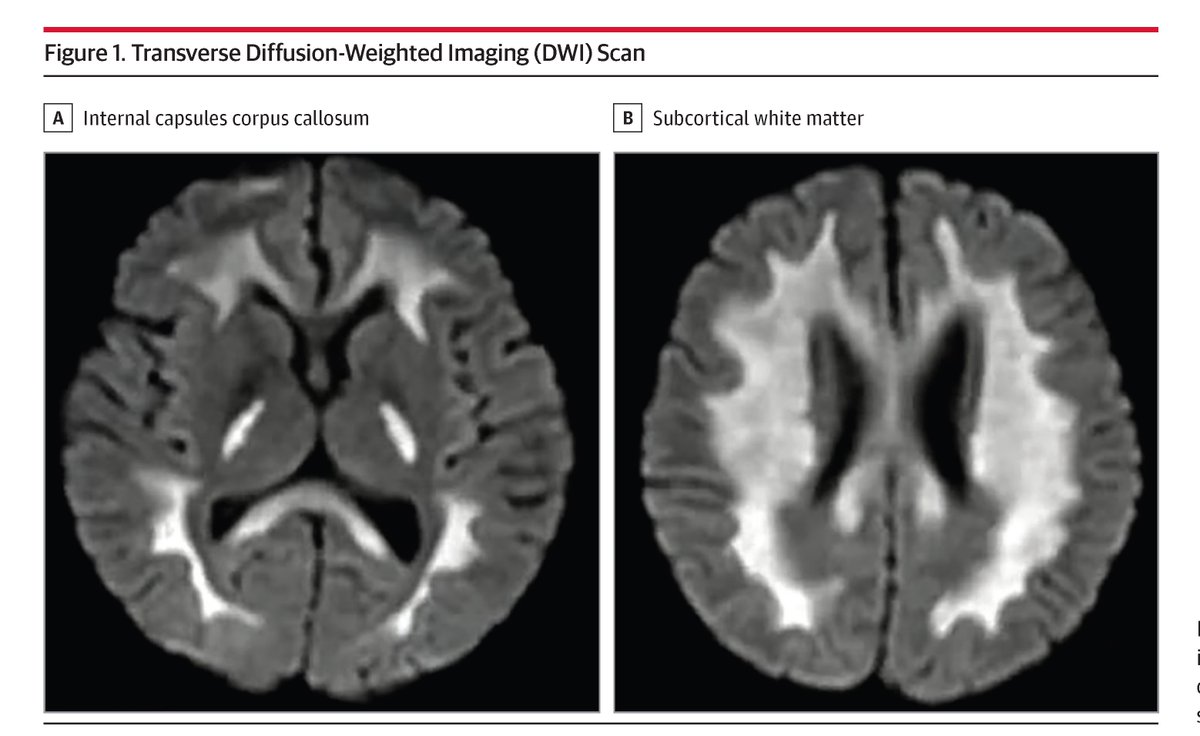
This case report describes a patient who presented with a 2-day history of dizziness, unsteady gait, and confusion. In the past month, he had experienced 2 cerebral infarctions and fungal infection in his left armpit. ja.ma/4uq01j1
English
Irake retweetledi
Interventional Radiology Basics - The Back Table
youtu.be/jwZZTAZlGdg Started a video series on Interventional Radiology procedure basics for med students and residents rotating on IR. This one explains the back table #futureradres #interventionaradiology #irad #iradres #meded

YouTube
English
Irake retweetledi
Irake retweetledi

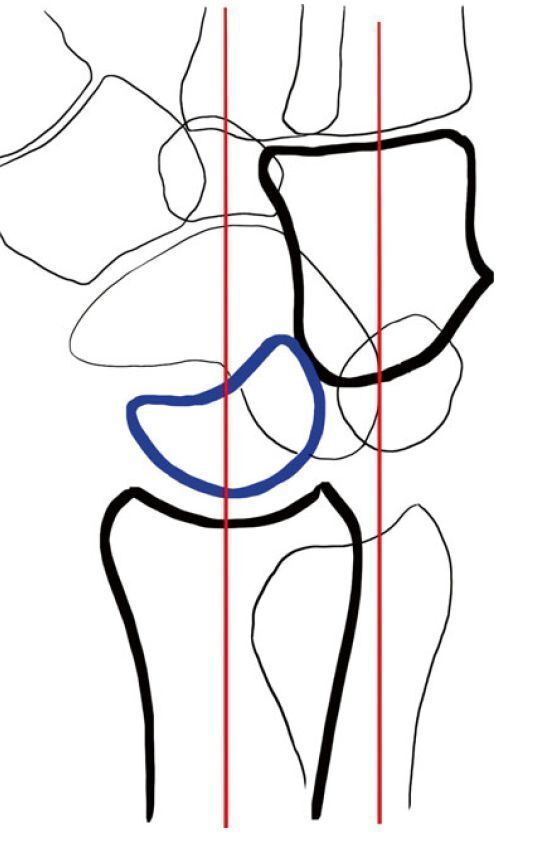
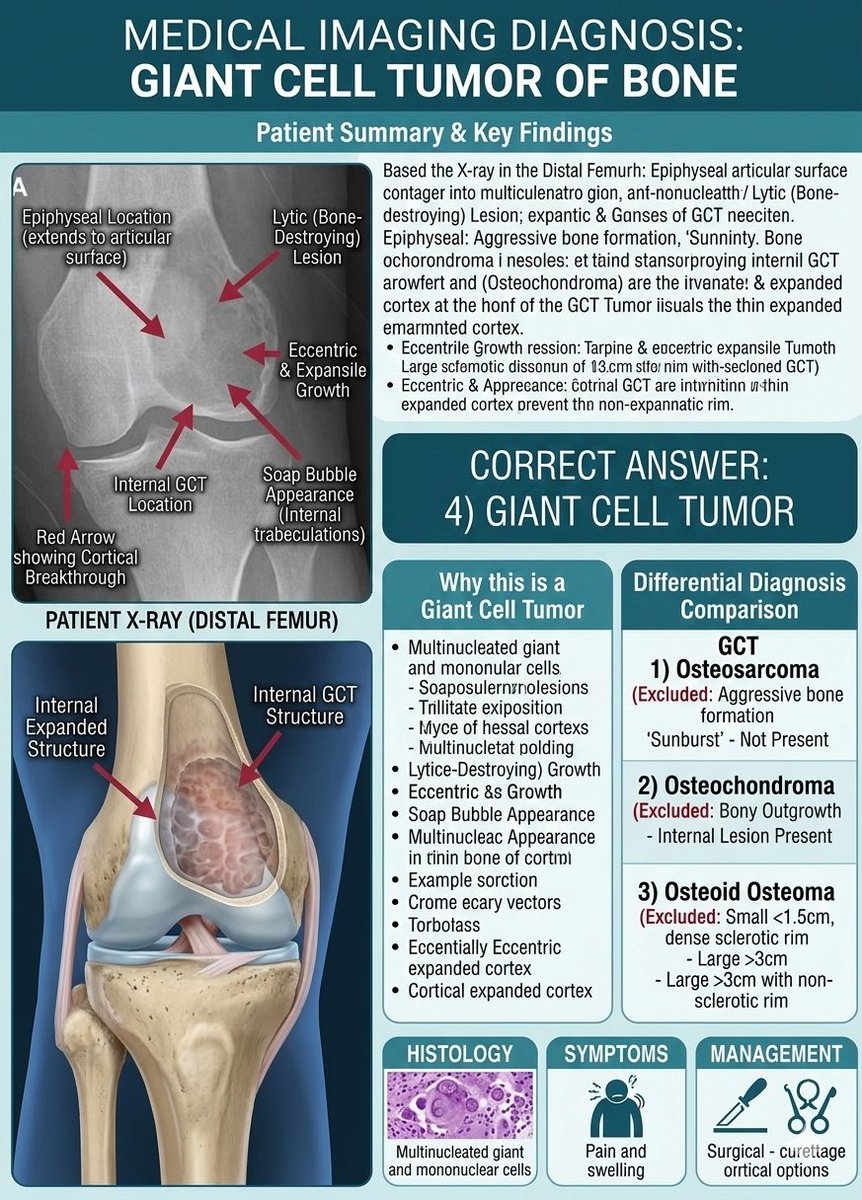
Answer:
4) Giant Cell Tumors.
#X_ray_Findings
• Location (Epiphyseal): The lesion is located at the very end of the bone (distal femur) and extends directly to the joint surface (subchondral bone). This is a hallmark of GCT.
• "Soap-Bubble" Appearance: The blackened, lytic (bone-destroying) area contains delicate internal lines (trabeculations) that look like bubbles.
• Eccentric Expansion: The tumor is off-center and is pushing the outer bone shell (cortex) outward, making it thin and fragile.
• No Sclerotic Rim: Unlike slower-growing benign lesions, there is no thick white border around the tumor, indicating its locally aggressive nature.
#Differential_Comparison:
• Not Osteosarcoma: It lacks the aggressive "sunburst" bone formation or Codman’s triangle.
• Not Osteochondroma: There is no bony outgrowth; the lesion is inside the bone.
• Not Osteoid Osteoma: The lesion is too large and lacks the characteristic small central "nidus" and dense surrounding bone.
#Note
Giant Cell Tumors are generally benign but locally aggressive. They can cause significant bone destruction and have a high rate of recurrence if not fully removed.
#MEDHM
Dr Motasem Al-Gradey@Mota55em
What's The Diagnosis? 1) Osteosarcoma 2) Osteochondroma 3) Osteoid osteoma 4) Giant cell tumors Please Correct answer #MedX @IhabFathiSulima
English
Irake retweetledi


🔴 New Medical Research Opportunity!
Medical Students, IMGs, AMGs, Residents, Fellows, & Physicians
6 narrative reviews and 5 systematic reviews/3 Meta-Analysis mentorship modules are scheduled for March/April 2026
Comment to receive info
English
Irake retweetledi
A 35 y/o woman with a history of SLE presented to the ED with epigastric tenderness with watery and blood-tinged stool. Exam revealed left–middle abdominal and epigastric pain. CT of the abdomen with contrast revealed severe long-segmental concentric wall thickening of the small intestine with submucosal edema (A, stars) and “bull's eye sign” (B, red arrows). Neither bowel ischemia nor perforation was found
Clinical images in ACR Open Rheumatology
doi.org/10.1002/acr2.9…

English
Irake retweetledi

What is the biggest 'gap' between residency training and real-world practice?
English
Irake retweetledi

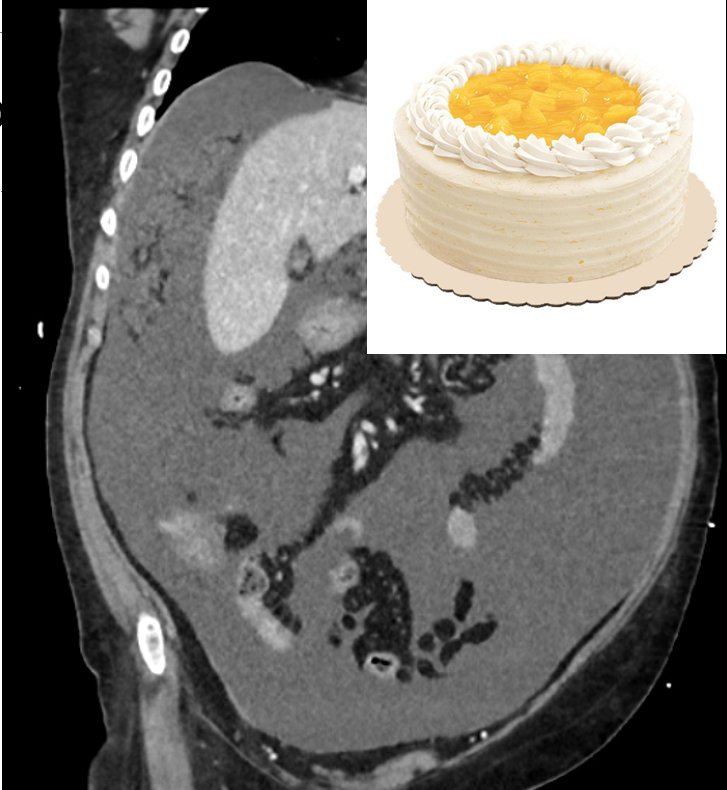
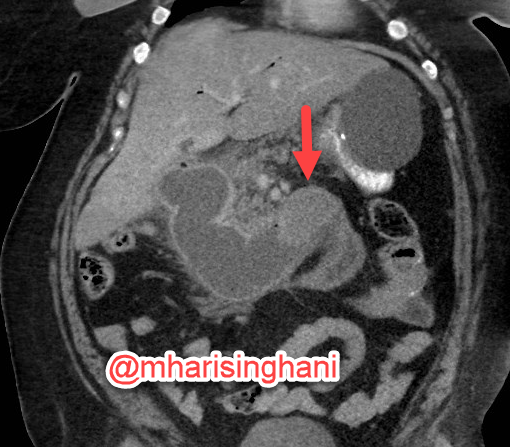
An 87 years old with abdominal pain and weight loss.
What is happening?
What is the radiological Sign?
What is the diagnosis?
English
Irake retweetledi

Bouveret syndrome; form of gallstone ileus, large gallstone passes through a bilioduodenal fistula, causing gastric outlet obstruction
English
Irake retweetledi
