DR F K
99.1K posts


DR F K
@Kemboy254
Surgery | A stoic wannabe
Nairobi, Kenya Katılım Haziran 2012
2.5K Takip Edilen5.3K Takipçiler

DR F K retweetledi

🚨⛔️ Jurrien Timber is out of Sporting vs Arsenal tomorrow, Mikel Arteta confirms.

English
Haha tactics za kishoga
Fabrizio Romano@FabrizioRomano
🚨⛔️ Bukayo Saka is OUT of Sporting vs Arsenal, Mikel Arteta has confirmed. ❌
Filipino
DR F K retweetledi
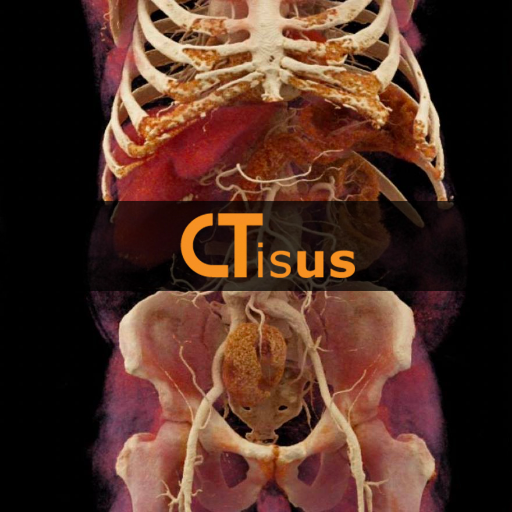
This review article provides a comprehensive description of the diagnostic and therapeutic strategies for treating Morel-Lavallee lesions.
@susan_kartiko; @Trauma_Q; #GW
journals.lww.com/jtrauma/fullte…

English


💙 Methylene blue in septic shock: miracle, myth… or misunderstood tool?
We all know the scenario:
👉 Refractory vasoplegic shock
👉 Escalating norepinephrine
👉 Vasopressin, steroids… still hypotensive
At some point, the question comes:
Should we use methylene blue?
⚡ Mechanism
Septic shock = NO-driven vasoplegia
Methylene blue acts by:
❌ Inhibiting nitric oxide synthase (NOS)
❌ Blocking soluble guanylate cyclase
⬇️ Reducing cGMP
➡️ Restoring vascular tone
👉 A true catecholamine-sparing strategy
📊 What does the evidence say?
Reality check:
Use in practice is rare (~0.5% of septic shock patients)
Often used as late salvage therapy
Dosing strategies = highly variable
But RCT signals are interesting:
↓ Vasopressor duration
↓ ICU / hospital length of stay
Possible ↓ mortality (low certainty)
👉 Evidence is promising… but still weak
🚨 The clinical dilemma
Timing is everything:
Early use → potential physiologic benefit
Late use → often too late to change trajectory
👉 Current practice is probably backwards
⚠️ What about safety?
Potential concerns:
Serotonin syndrome (with SSRIs)
Pulmonary vasoconstriction
G6PD-related hemolysis
Interference with pulse oximetry
👉 Most serious effects seen with high doses
🧠 Take-home message
> Methylene blue is not a “magic drug”
but it may be a physiology-driven adjunct in vasoplegic shock
❓The real questions are:
Who benefits?
When to give it?
At what dose?
🚀 Where we’re heading
Ongoing trials (e.g., BLUSH trial) will clarify:
✔️ Early vs late use
✔️ Optimal dosing strategy
✔️ True impact on mortality
👉 This could redefine vasoplegic shock management
💡 Clinical reflection
Next time you face refractory shock, ask:
👉 Is this still “fluid + catecholamine problem”…
👉 or already a NO-mediated vasoplegia problem?
📚 Reference
Fernando, S. M.et al. Journal of Critical Care, 92, 155353.
doi.org/10.1016/j.jcrc…

English
DR F K retweetledi


Hahaha.... partly true.
But because we are used to mediocrity it sounds weird.
Ngazekof🇰🇪@Mghazake
Students who did 3 sciences in highschool used to tell us that a D in physics is better than an A in history😂
English
DR F K retweetledi

DR F K retweetledi



Maliza hao wote, na their minions, fcvkers!
AFTV@AFTVMedia
Arsenal Women are out of the Women’s FA Cup. 😔
English
DR F K retweetledi

An interesting finding in the liver. What do you think has happened here?

English
DR F K retweetledi


DR F K retweetledi

As a continent, we are collectively foolish
Instablog9ja@instablog9ja
Borehole engineer shares how he locates water underground.
English
DR F K retweetledi


Me reading this 50/50 story as the man of the house is making dinner
GIF
English
Stinging display of opulence
Rodgers Kipembe Mpuru@RodgersKipembe
Lakini mbona Premio iuzwe KSh. 2.7 Million?
English
Aesthetics improved by Halloween mask, the first of it's kind.
KENYA GOSSIP CLUB@kenyagossips
Rapper Stevosimpleboy Rocking A Unique Outfit For Easter. Rate It Out Of 10 😅
English