Is low-dose quetiapine safe for insomnia?
Nope. Weight gain and dyslipidemia still there, not to mention tardive dyskinesia:
pubmed.ncbi.nlm.nih.gov/40772433
It deepens sleep quality, but I'd use only if needed for another disorder like depression, bipolar, or schizophrenia.
Controversial take: I think of addicts and alcoholics as more “facers” than “avoiders.” Their coping skills are dysfunctional and destructive, but they’re still actively trying to change how they feel
@TweetATherapist so you use the shift in concept, to reduce shame, and enhance harm reduction. in short the message you "you are active in trying to help yourself, not avoidant, you have the power to continue to be active, you are a FACER"
Is that it?
@KemtrupTweets 3. the difference between work responsibility and as you said well PLAY/free time
4. Exercise alone is not a treatment for anything. Nothing works alone. Exercise or diet or ssri or behavioural activation or psychotepy cannot and do not work alone …
@KemtrupTweets How I present exercise
Exercise is not the same as physically demanding work
It is a lifestyle change. A moment you give yourself to exist, to matter and to get better. It allows you to have social connection with people who see the world similarly…
@JRBneuropsiq@chrisaikenmd Sorry for the many questions but it’ll definitely help a young clinician like me! How do you choose between celocoxib v a typical augmenting agent like bup v pramipexole?
Inflammation is common in late life depression, concludes new review:
ncbi.nlm.nih.gov/pubmed/40709634
We are learning more about how to personalize therapy for inflammation (hs-CRP > 3). Anyone testing CRP in practice?
[Table from my upcoming book on Difficult to Treat Depression]
@LElkrief@chrisaikenmd To me, it has many advantages:
1) providing a better explanation (to patients) about the cause of symptoms like pain, fatigue, etc
2) opening the door to a more thorough investigation of the cause of the inflammation
3) selecting pharmacotherapy
@chrisaikenmd@JRBneuropsiq So high CRP, we look for other factors listed on your table and treat accordingly with best fitting option? I will try out in next few months!
@LElkrief@JRBneuropsiq Good question. The meds that work better in inflammation are in the post. Also points to some natural therapies, and it influences the dosing there (like higher doses of omega-3 and exercise are needed during inflammation)
@JRBneuropsiq@chrisaikenmd How would it change your approach ? Say 70 year old TRD presents with refractory depression. Say you find the elevated CRP, what would you do different
@chrisaikenmd I do test for CRP in clinical practice. I think it's useful to identify the subset of patients with depression who have low grade inflammation
I am not your doctor so don’t take this as medical advice…
But if there were only one supplement to consider taking for your 🧠, 💪🏻, and mental health …
Creatine monohydrate wins
5g each am in coffee (heat helps dissolve)
10g when sleep deprived
Don’t take for bipolar
@awaisaftab Exactly. To me it is the job of the modern day psychiatrist to shift the focus from sx to problems (stories), while keeping the sx in mind to make it easier to find solutions to the problems.
When it comes to interviewing new psychiatric patients in my clinic, I am fascinated by how some people are very focused on their symptoms (depression, anxiety, panic, irritability, mood swings, inattention…) and some people are very focused on their stories (‘I went through divorce/break-up/death/work conflict, and I am overwhelmed, struggling, unable to function’)…
And sometimes I have patients who start off by being very symptom-focused, and then as treatment progresses, they start becoming more and more story-focused, and when that happens, it is usually a sign of clinical improvement.
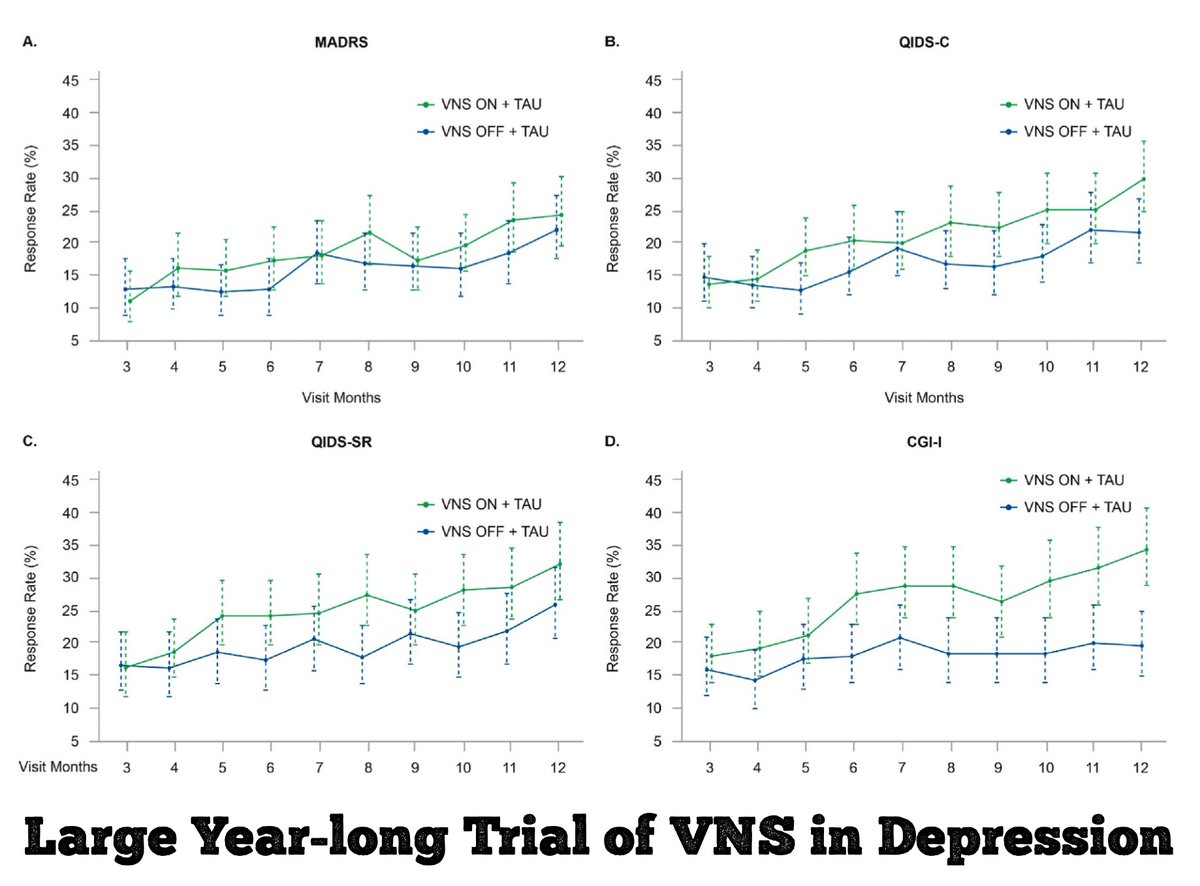
Here's a rarity. A 12-month sham-controlled trial of vagus nerve stimulation (VNS) in 493 adults with high degree of treatment-resistant depression.
Unfortunately, results were equivocal, failing on primary outcome but passing on secondary ones:
pubmed.ncbi.nlm.nih.gov/39706521
@chrisaikenmd I have reservations with the patient population. Avg t of current ep was above 10 years … is this a dysthymic pop? A pop with difficult to treat personality styles/disorders?
VNS works best (in my view) when there are clear beginning and end to depressive pathology in history.
This is a significant step towards creating evidence-based, transparent decision-support tools for clinicians and legal professionals. A must-read for anyone interested in #AI, #ForensicPsychiatry, or #MentalHealthLaw. Congrats again to Dr @AlexandreHudon !
What’s really impressive is the model's accuracy (98.1%) and its interpretability. It can pinpoint which factors—like the patient's age or the severity of their diagnosis—most influence the outcome. This transparency is key for ethical AI in sensitive fields.
Excited to share this new paper by my colleague, Dr. @AlexandreHudon , published in @FrontiersInAI! He's developed a hybrid AI model to predict outcomes for psychiatric treatment orders—a crucial issue at the intersection of healthcare and law. ⚖️🧠🧵
frontiersin.org/journals/artif…