Sabitlenmiş Tweet

If you’re interested in learning, staying updated, and exploring medicine in a simple and practical way, I’d be happy to have you there.
Your follow and support mean a lot. Thank you!
English
Dr M.AL-gradey
1.3K posts

@MAbdullah58266
Medical Doc,Health content, follow for medical CASES &MCQS daily Medical pearls Questions alternative account

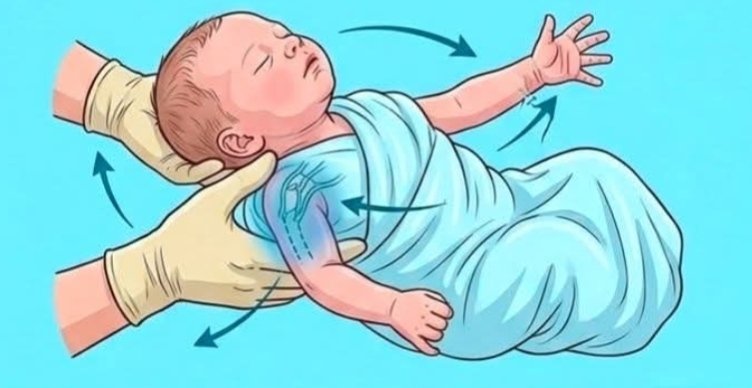
A newborn with weak Moro reflex on one side after difficult delivery may have❓ A. Erb’s palsy B. Hydrocephalus C. Neonatal sepsis D. Hypoglycemia







What is the diagnosis ⁉️








Came in for stroke like symptoms. What's the diagnosis?🤔 @IhabFathiSulima