Mona vijayaran retweetledi

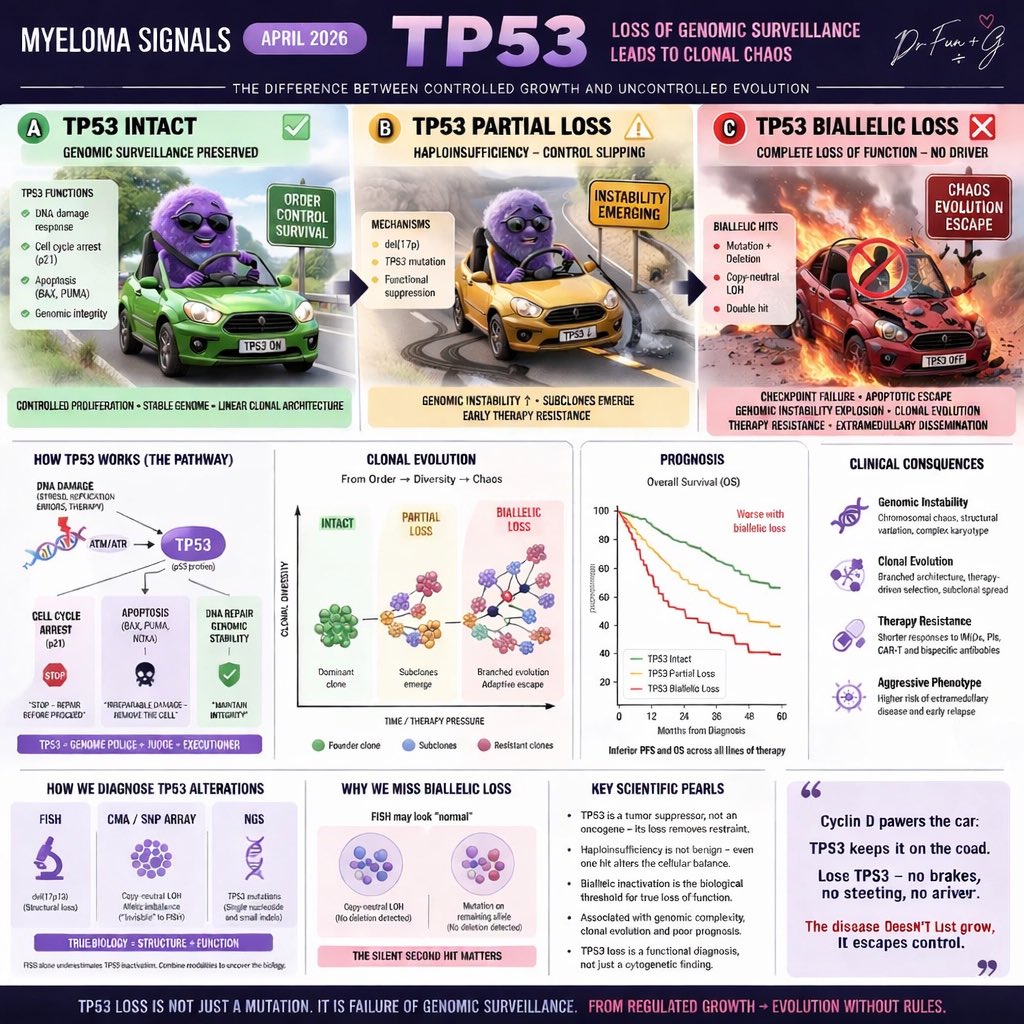
Myeloma Signal: TP53
TP53 is the guardian of genomic integrity.
Cyclin D powers the cell.
TP53 keeps it under control.
Monoallelic loss:
→ genomic instability begins
→ subclones emerge
Biallelic inactivation:
→ checkpoint failure
→ clonal evolution accelerates
→ therapy resistance dominates
This is not just high-risk disease.
This is evolution without control.
English