Michael Weisman retweetledi

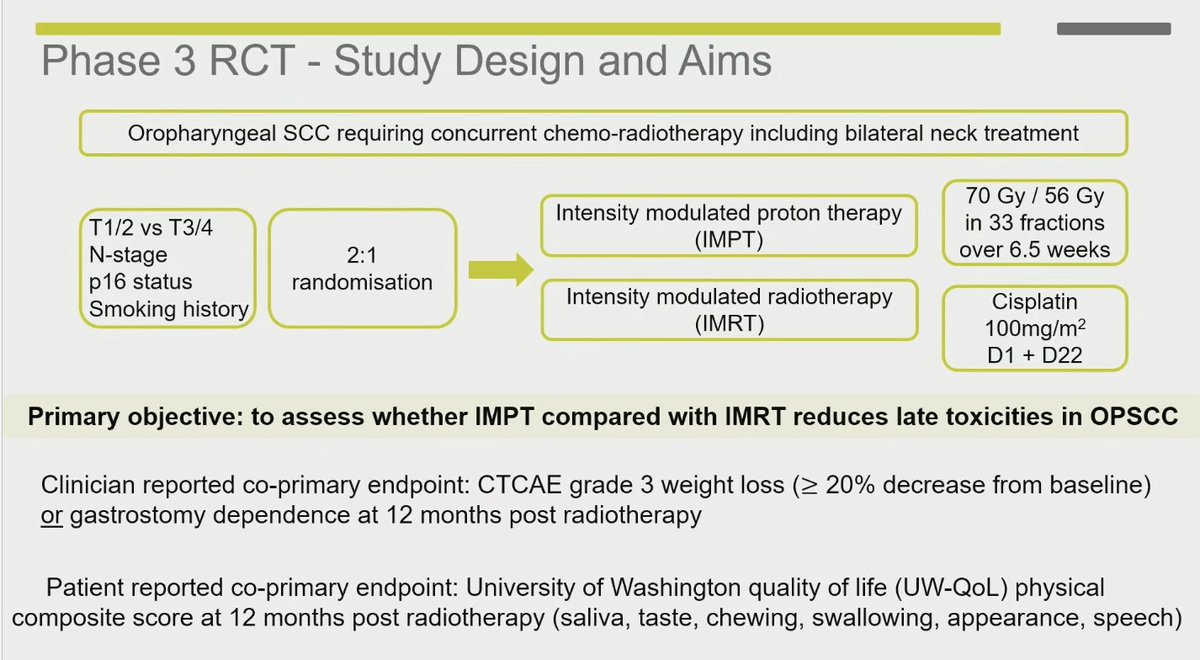
🧵 Just published in @TheLancet: TORPEdO – the first phase 3 RCT designed specifically to test whether IMPT (proton beam) improves late function & QoL vs modern IMRT in oropharyngeal SCC.
Short answer: It doesn’t.
Long answer (with the numbers that matter) 👇
English