Sabitlenmiş Tweet

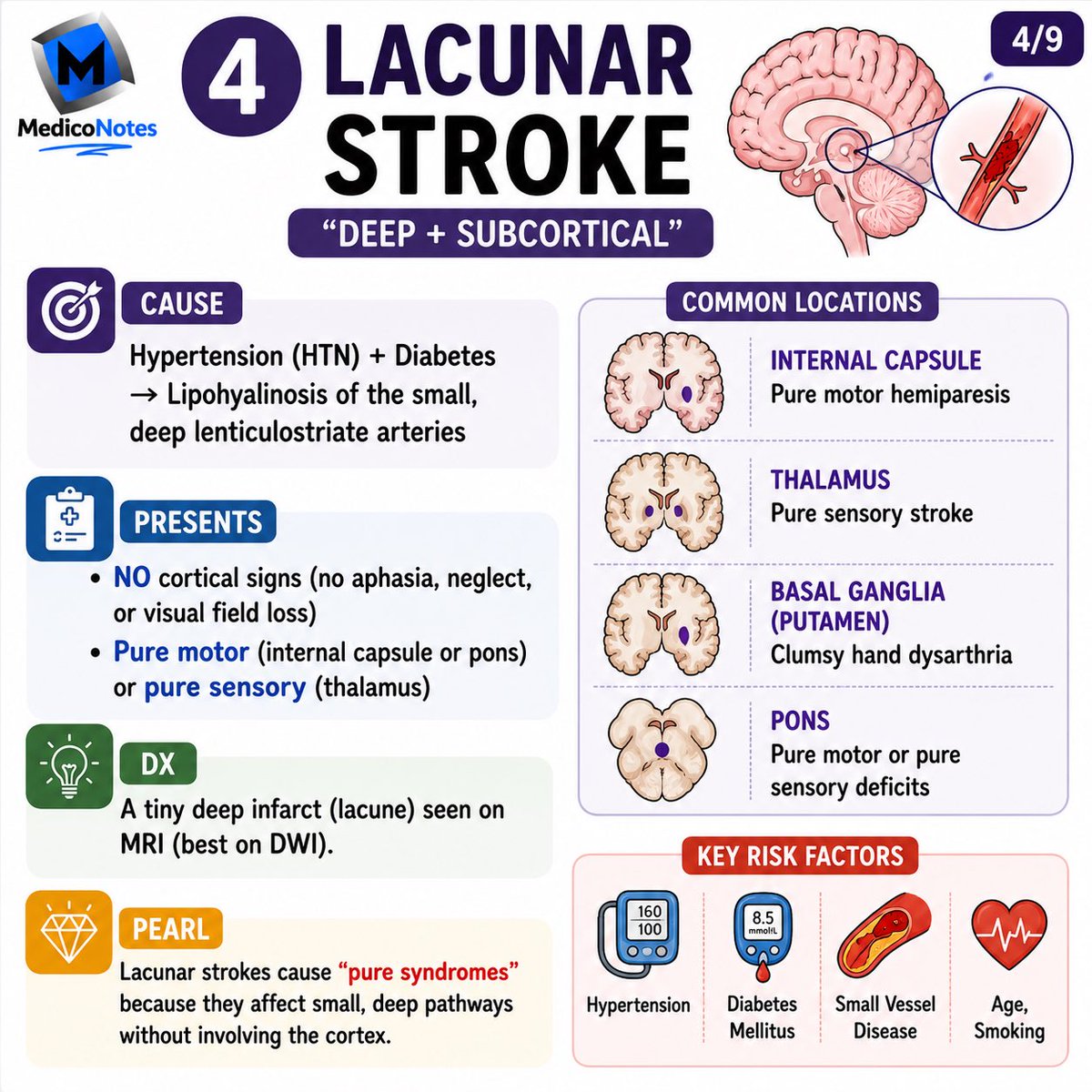
MedicoNotes is an online medical education platform that provides professionally designed high-yield medical notes to help doctors prepare for exams and excel in medical practice.
💡 Study smarter with our medical notes and improve your exams results!
👉 A MUST-HAVE for all Medical, MBBS, MD, & MBChB students, PA, nursing students, as well as professional exams including USMLE, PLAB and UK Royal College exams.
👉 ALL Notes are delivered instantly in print-ready PDF format so you can study the way you learn best!
👉Free sample downloads are available at our website: mediconotes.com
———————-
#medstudentnotes #medstudent #medicalstudent #MDstudent #studentdoctor #medicine #medicalschool #medschool #medicalnotes #doctors #premed #futuredoctors #usmleprep #usmle #medstudentlife #medstudy #mednotes #medicalstudy #medicalnotes #medico #PAstudent #MDlife #mbchb
English