Michael Mao, M.D. retweetledi
🔦✅Fibrillary Glomerulonephritis (FGN) : Classic Diagnostic Features
Renal biopsy: Mesangial expansion + irregular capillary wall thickening with PAS-positive, silver-negative deposits. Congo red negative.
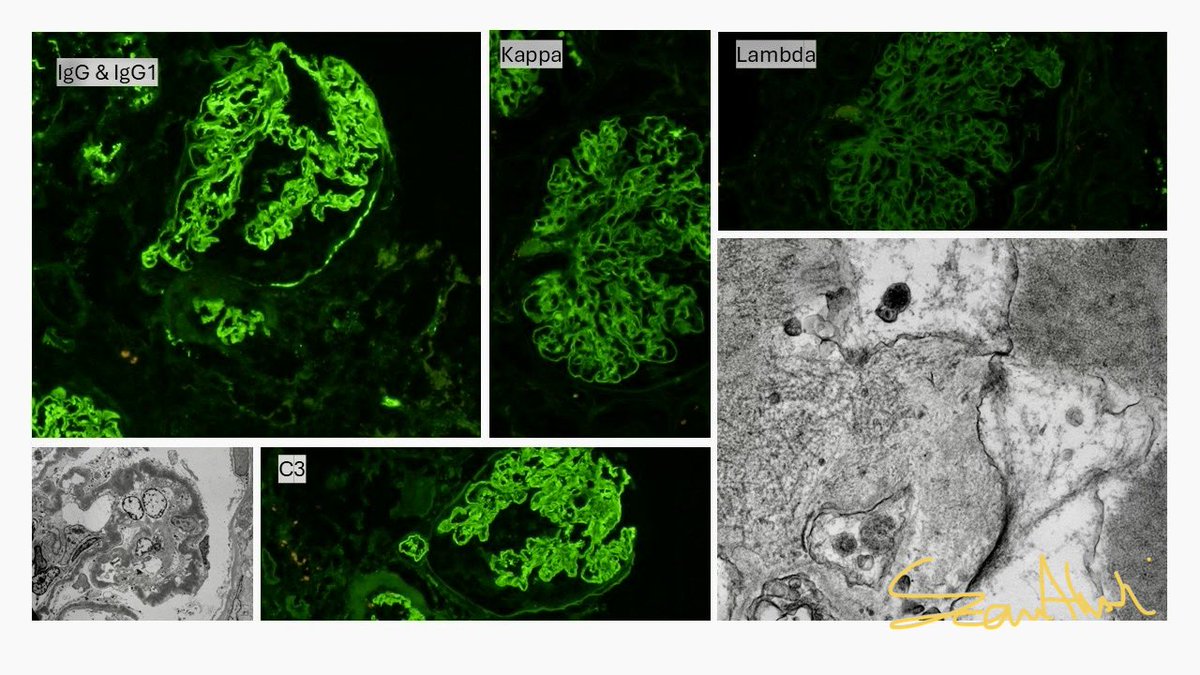
🔬 Immunofluorescence (IF) (classic polytypic pattern):
- Bright IgG (often IgG4 > IgG1, polyclonal)
- Both κ and λ light chains positive (no restriction)
- C3 positive (often 2–3+)
- Variable IgM/IgA (usually weak/negative)
⚡ Electron Microscopy (EM) : pathognomonic:
- Randomly oriented, straight, non-branching fibrils (mean ~18–22 nm diameter, range 12–24 nm)
- No hollow centers (distinguishes from immunotactoid GN)
- Deposits in mesangium, GBM, subendothelial ± subepithelial spaces
🧬 DNAJB9 immunohistochemistry:
- Strong, diffuse glomerular positivity (mesangial + capillary wall) , highly sensitive & specific (>95%) for FGN
- Now considered the gold-standard confirmatory marker (revolutionized diagnosis even when EM is unavailable)
🔦✅Monotypic (monoclonal-appearing) FGN:
- Rare subset (~3–11% of cases)
- Shows light-chain restriction (e.g., lambda or kappa) ± IgG subclass restriction (often IgG1)
- Most DNAJB9+ monotypic cases do NOT have detectable circulating monoclonal gammopathy or underlying plasma cell/lymphoproliferative disorder (paraffin IF often needed to confirm true monoclonality)
- Still evaluate for paraprotein-related disease (SPEP/UPEP, bone marrow, etc.) in monotypic cases @MayoClinicNeph

English