Sabitlenmiş Tweet
Nephro
938 posts

Nephro
@Nephro18
Nephrology enthusiast | Simplifying complex kidney science into digestible insights | Follow for summarized nephrology articles and updates #Nephrology
Washington, DC Katılım Eylül 2021
1.1K Takip Edilen840 Takipçiler
ADPKD—Kidney replacement therapy (Dialysis)
📍Dialysis modality choice = shared decision-making
📍Choose HD vs PD based on patient factors + patient choice + facility availability (2C)
📍No survival difference between PD & HD.
📍PD is a viable option in ADPKD kidney failure ✅
▪️Use caution only if massive kidney/liver enlargement or other standard PD contraindications
📍HD prescription + supportive care (e.g., anticoagulation) = same as non-ADPKD
📍Evidence summary (PD vs HD in ADPKD):
▪️Mortality: no significant difference (
▪️On PD (ADPKD vs non-ADPKD): no significant differences in Kt/V, peritoneal leaks, peritonitis, switch to HD, technique failure, exit-site infection, or mortality
▪️Hernias: more common in ADPKD on PD
▪️Median technique failure: 6.2 yrs (ADPKD) vs 6.5 yrs (non-ADPKD)
▪️Median time to death: 6.04 yrs (ADPKD) vs 5.57 yrs (non-ADPKD)
▪️More switching PD → HD
▪️One study: hospitalization for infection higher with PD vs HD (58% vs 44%); possible ↑ hernia surgery (7% vs 4%)
English
Cont. ADPKD—Kidney transplantation cont
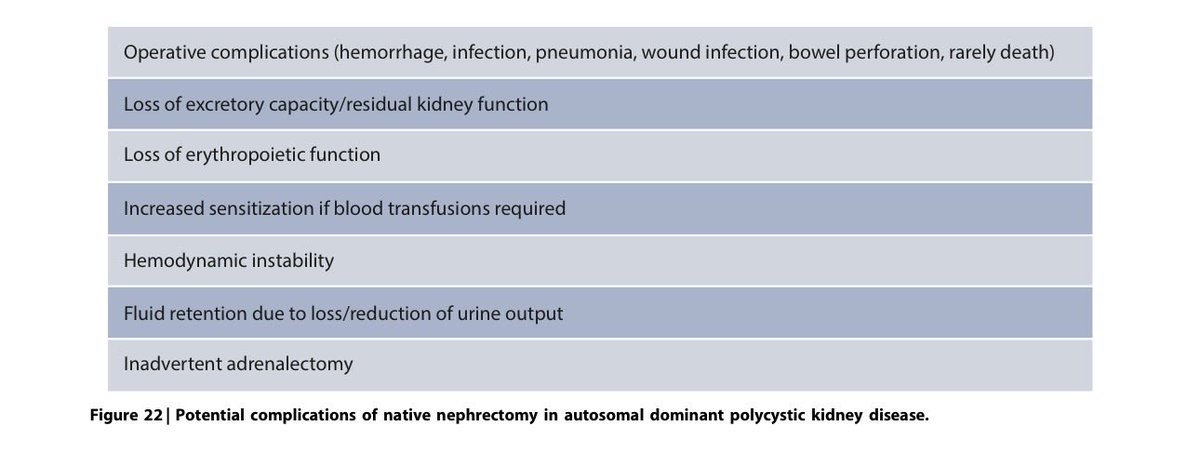
⚫️Nephrectomy
📍 Native nephrectomy NOT routine
▪️do only for specific indications when benefit > risk (2C)
▪️ 9 studies—no clear benefit for graft loss or all-cause mortality after Nephrectomy
▫️possible higher transfusion risk if nephrectomy done at time of transplan
▫️note kidneys often shrink up to ~30% in 1st year post-Tx (may improve symptoms)
📍Prefer unilateral over bilateral nephrectomy when appropriate (2D) ✅ (lack of benefit for bilateral + concern for higher complications, e.g., refractory hypotension)
📍Pre-Tx nephrectomy: meta-analysis shows near-significant ↑ long-term mortality; large database suggests ↑ in-hospital post-Tx death
📍Consider longer operative time + transfusion risk → individualized planning
📍 Timing when nephrectomy needed 🕰️: suggested at time of or after transplant, not before, whenever possible (2C)
📍 Surgical approach 🔧:
▪️when feasible, hand-assisted laparoscopic over open nephrectomy (2D) ✅ (similar complications overall, less transfusion)
⚫️(RCC screening pre tx):
📍Individualize RCC evaluation; consider kidney imaging (e.g., abdominal MRI) within 1 year before anticipated transplant
📍Most studies: significant RCC risk not increased vs other etiologies
▪️some cohorts suggest increased RCC in ADPKD
📍Prefer noncontrast MRI in kidney failure/dialysis
▪️give gadolinium (group II) only if necessary
📍MRI advantages:
▪️better soft tissue
▪️can classify simple vs hemorrhagic/proteinaceous cysts
▪️solid lesions have intermediate signals + DWI helps
📍if solid lesion suspected (not AML), consider contrast for enhancement/staging; CEUS possible but often limited in ADPKD due to size/multiplicity
English
Nephro retweetledi

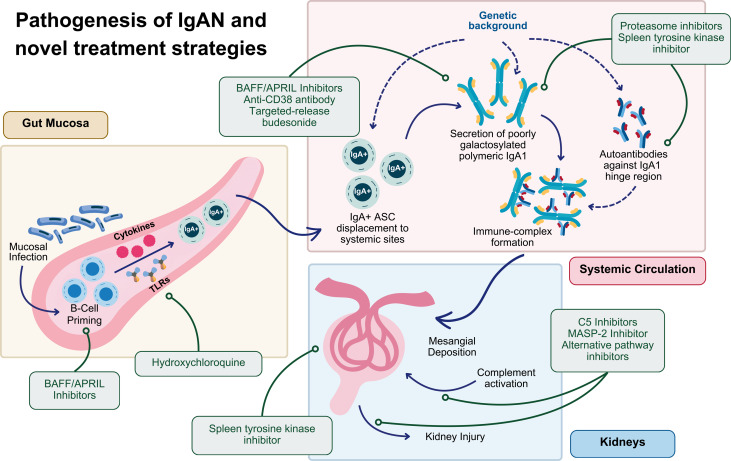
IgA Nephropathy #IgAN: An Overview of the Clinical Trials ca. 2025 from @KidneyMed @ZohrehGh7 @haresh11 @NWiegley @Alexgr23 @rahaai @SaynaNorouzi @JEGAYTAN90
#Nephpearls
👉 kidneymedicinejournal.org/article/S2590-…
English
English
Are you attending #ISNWCN? Join us for the KDIGO session:
📌 IgA Nephropathy in 2025: Bridging the Gap Between Knowledge & Practice
🗓️ Saturday, February 8, 13:00-14:00
📍 Amaltas B Hall – B101B
📺 Livestream: #industry-symposia-saturday" target="_blank" rel="nofollow noopener">theisn.org/wcn/industry/l…
Moderated by Liz Lightstone, the session features Hernán Trimarchi on #IgAN pathophysiology, diagnosis, prognosis & global implementation.
Brad Rovin will present case-based treatment strategies, followed by a 15-minute Q&A-- a great opportunity to learn & engage.
We hope to see you there! #WCN25 🇮🇳
English



1/Radiologist not answering the phone?
Just want a quick read on that stat head CT?
Here's a little help on how to do it yourself w/a thread on how to read a head CT!

English
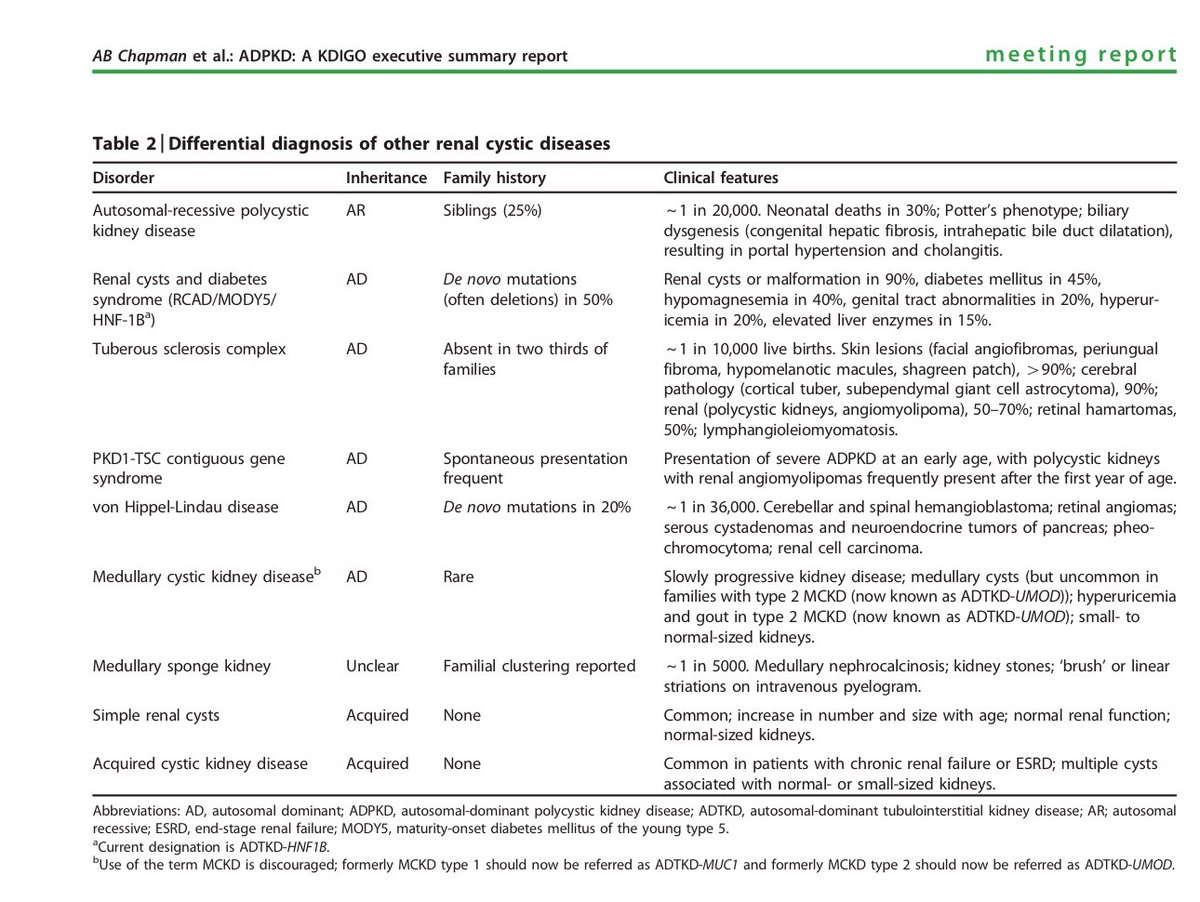
Differential Diagnosis
▪️Acquired Kidney Cysts: ↑ with age, no family history
•0% (15-29 yrs)
•1.7% (30-49 yrs)
•11.5% (50-70 yrs)
•22.1% (≥70 yrs)
•Bilateral cysts rare <50 yrs
▪️ Localized Cystic Disease: Single kidney, no family history, non-progressive.
▪️ Acquired Cystic Kidney Disease: Small bilateral cysts in CKD, ↑ risk of RCC, normal/small kidney size.
▪️ Drug/Metabolic Cysts: Lithium, crizotinib, dRTA, Carney complex, rickets.
▪️ Collagen Mutations: HANAC, thin basement disease → cysts + microhematuria.
▪️ Parapelvic Cysts: Lymphatic cysts sparing cortex (≠ADPKD).
▪️ Medullary Sponge Kidney: Medulla cysts, stones, nephrocalcinosis, normal cortex.
▪️ Genetic Cystic Diseases:
•ARPKD
•TSC: Angiomyolipomas, facial signs.
•VHL: Cysts + retinal, clear cell cancer.
•ADTKD: Small kidneys, gout.
•HNF-1B: Cysts + systemic signs.
•OFD1: Cysts + oral, facial, digital anomalies.
English
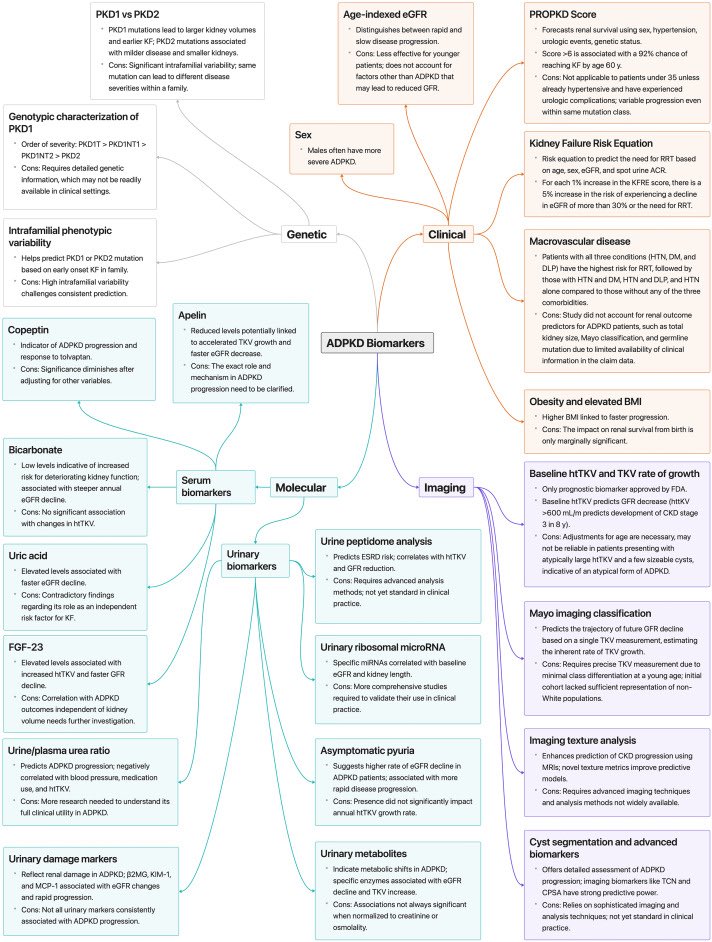
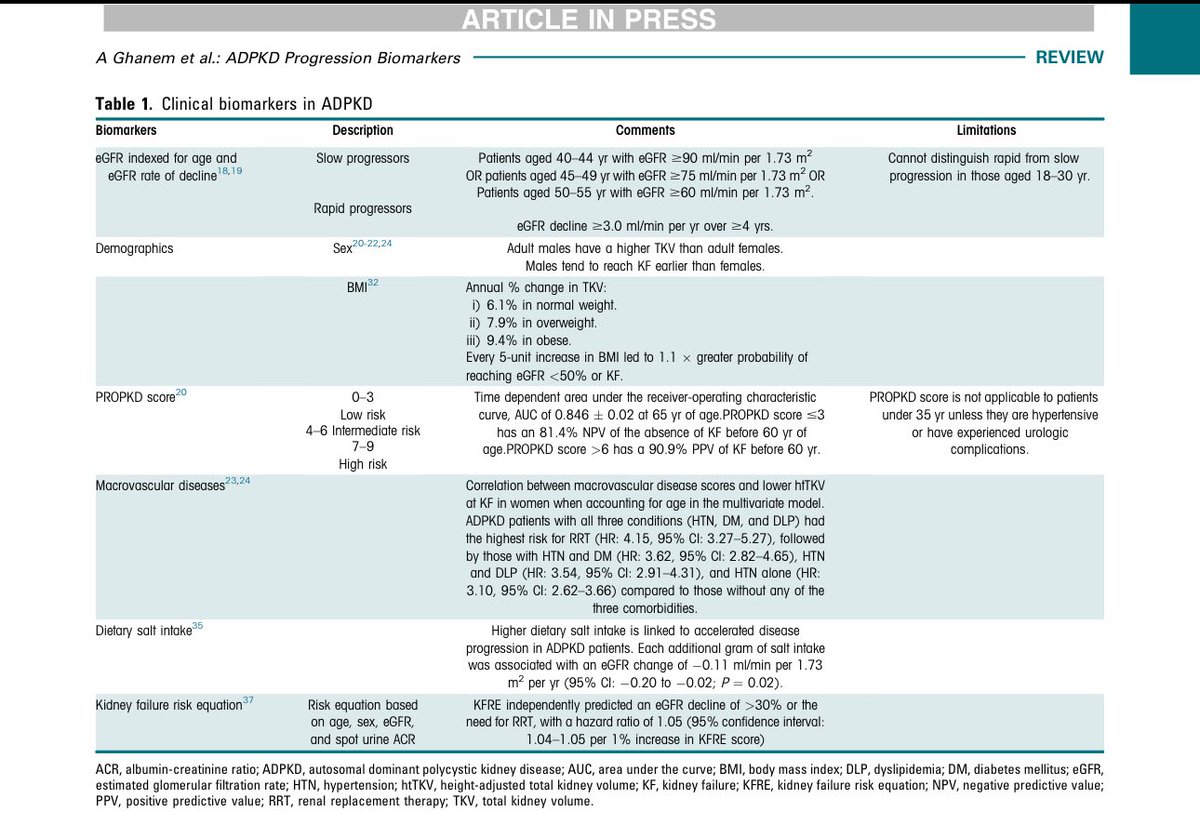
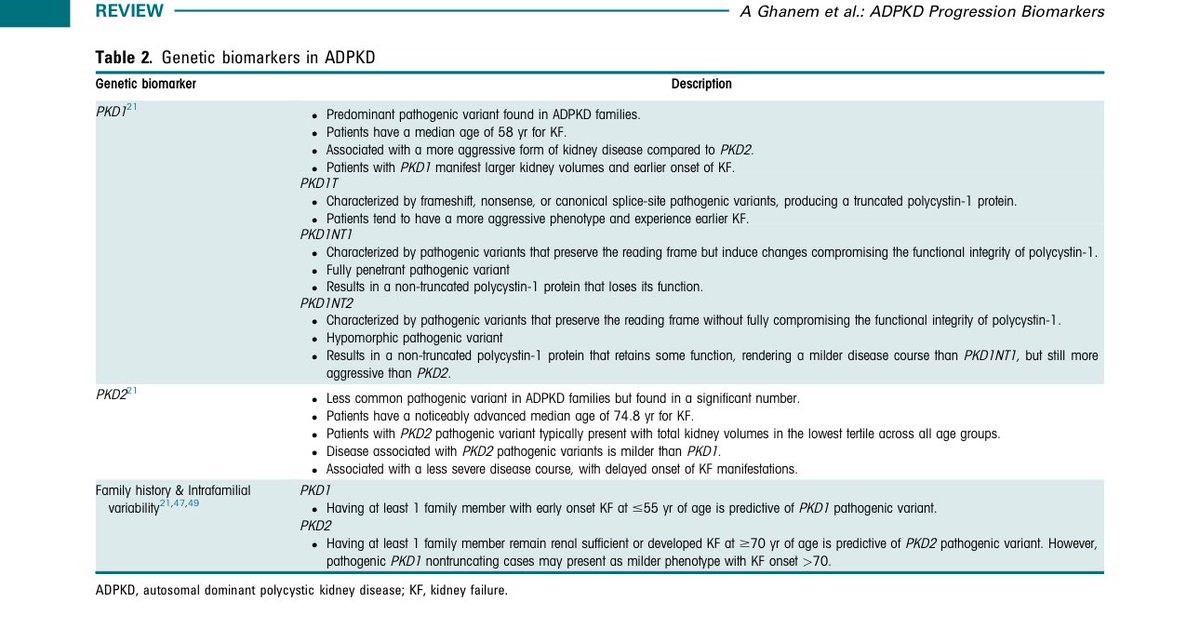
Here’s a comprehensive review of biomarkers of kidney disease progression in adults and children with ADPKD
@fouadchebib
📍eGFR → Indexed for age, identifies rapid vs. slow progressors.
📍Sex → Sex: Males have ↑ TKV, more severe ADPKD, reach KF ~5 yrs earlier.
📍PROPKD score → Combines sex, HTN, genotype for KF risk stratification.
📍BMI → ↑ BMI linked to faster TKV growth and eGFR decline. visceral fat is a better predictor of progression.
📍Macrovascular Disease → ↑ HTN, stroke, CV disease with age = faster kidney decline.
📍Salt Intake → ↑ intake → ↑ eGFR.
📍KFRE → Predicts eGFR decline or RRT need using age, sex, eGFR, ACR.
📍TKV/htTKV → predicts CKD 3 within 8 yrs, early predictor of ↑ GFR .
📍Mayo Imaging Classification → htTKV + age classify rapid progressors (1C-1E) with faster GFR decline.
📍Imaging Texture → Features like entropy improve prediction of CKD stage 3
📍Cyst Segmentation → Biomarkers like TCV and CPSA predict disease progression.
📍PKD Genotype → PKD1/PKD2 variants impact disease severity and KF onset.
📍Serum Bicarbonate → Lower levels predict faster progression.
📍Copeptin → ↑ levels linked to ADPKD progression and response to tolvaptan.
📍Serum Uric Acid → ↑ levels predict faster TKV growth and KF onset.
Urinary Inflammatory Markers →
📍Biomarkers like MCP-1, KIM-1 predict damage and progression.
📍Urine Metabolites → PKM2 and cAMP tied to progression.
📍Tubular Secretion Markers → Impaired secretion linked to fibrosis and progression.
📍Urine-to-Plasma Urea Ratio → Predicts urine concentrating defects and faster progression.
📍Asymptomatic Pyuria → Linked with earlier KF and faster ↑ eGFR.
English