Sabitlenmiş Tweet

Published today✨
Real-world safety data for targeted-release budesonide (Nefecon) remain limited.
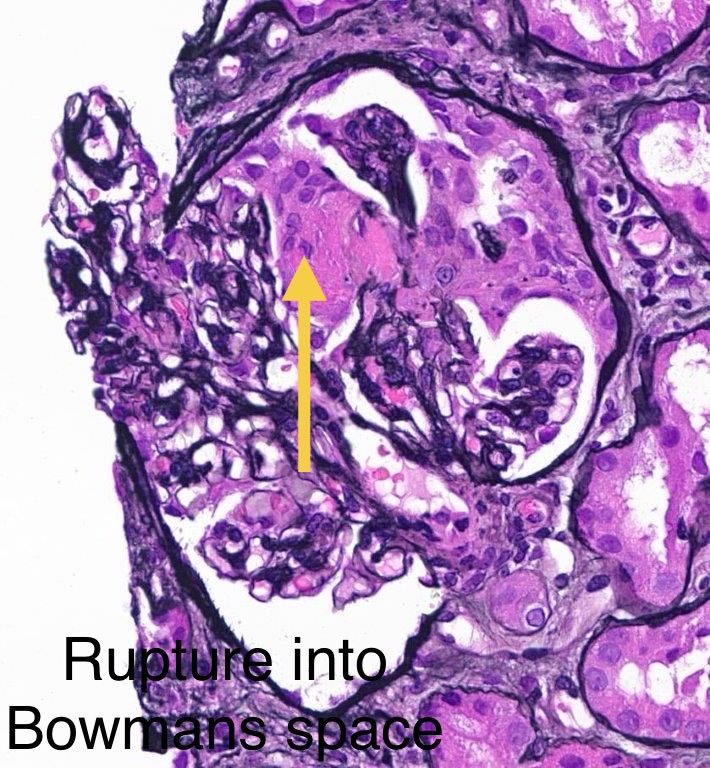
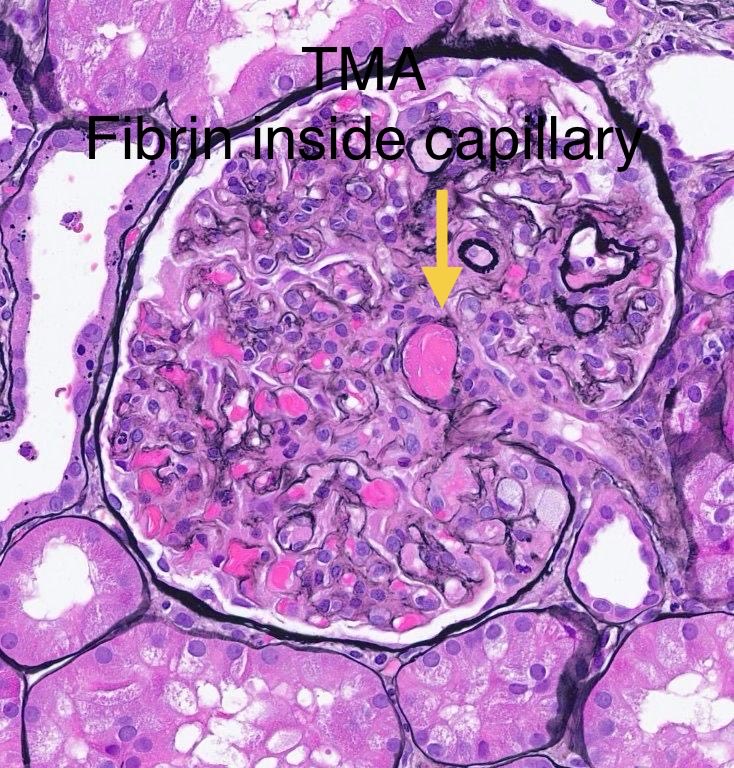
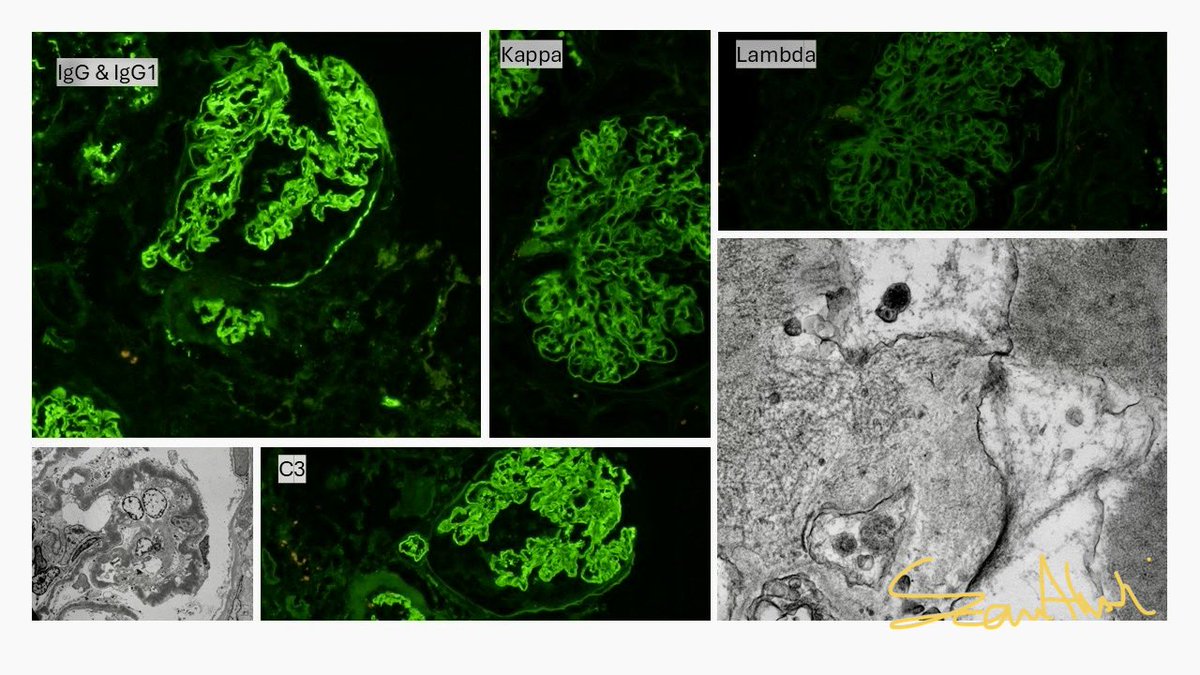
We report a case of IgAN w/ significant systemic adverse effects associated w/ Nefecon — highlighting the need for close monitoring.
@LadanZand @GlassockJ
doi.org/10.1093/ckj/sf…
English