
Mauricio Lema-Medina
7.4K posts

Mauricio Lema-Medina
@OncoNerd
La minga flash es la segunda mejor posible.
Medellín Katılım Ocak 2012
123 Takip Edilen2.9K Takipçiler

@MushtaqBilalPhD Thank you. Will certainly avoid if starting next February 30.
English

Sci-Hub is an evil website that pirated 85M+ research papers and made them freely available
And now they've added AI to their database to make Sci-Bot.
It answers your questions using latest, full-text articles.
But DO NOT use it. We should all try to make billion-dollar academic publishers richer.
I'm putting the link below so you know how to avoid it.
English
@jasonryanmd So, when they forget the actual vector they know what vector is.
English

What’s the point of testing super detailed memorization on medical boards in the age of AI and smart phones? I can look up that the sandfly is the vector of leishmaniasis in 20 seconds. Why test whether students have this memorized? We force trainees to spend hours memorizing factoids instead of learning other things that would benefit patients and the medical profession more. Am I missing some benefit of memorization in the modern era?
English
Qué bueno ver a un colombiano avanzando la ciencia - elcolombiano.com/tendencias/inv…
Español

Entrar a un edificio en Colombia es una experiencia inmersiva: parquee en reversa, firme 3 planillas, registre el código serial del computador, deje un documento en portería, lea el habeas data, vea el video de evacuación y casi casi, piden fotocopia ampliada de la cédula… todo para subir a una oficina en el piso 2. 🇨🇴
Español

Nadie habla de la estafa de las universidades élite de Bogotá: 24 millones de pesos el semestre, 2 horas de clase al día, 0 lecturas, 0 trabajos o análisis en casa, y cuando el profesor en hora de clase tiene que ir a la Feria del Libro, simplemente cancela y ya.
Español
@CrakerMc @pablosenabre Sería genial. No un asno que se niega a aceptar los avances. Siga con el ábaco.
Español

@OncoNerd @pablosenabre ¿Sabes lo que estaría genial? Que te tocase un cirujano primerizo que se haya sacacado el título con la IA.
Español

Lo último que me esperaba de mi semana era darme cuenta de que mi profesor está metiendo prompt injection en los PDFs de las prácticas para pillar a los que las hacen full con IA…
y que estaba cayendo TODO el mundo
Español
Inicio la serie sobre cáncer escamocelular de cabeza y cuello - parte I: principios generales - open.substack.com/pub/lemasobrec…

Español
@elcolombiano Sobre su interesante "De Santa Fe a Medellín: la disputa por ser capital que involucró hasta al amor", me queda una duda: Cómo las cuencas de los ríos Nare y Nus influyeron en el desarrollo de Medellín, cuando ninguno de los dos está cerca?
Español

A recent survey of 376 healthcare professionals revealed that 63% DID NOT understand the concept of a p-value.
Do you think you can pass the P-value explanation test❓
Are you part of the 63%?
Let's break it down in simpler terms…

English


@ELTIEMPO En Medellín mataron a tiros a otro urólogo que desgració la vida de un joven, John Ferney Cano González que terminó suicidándose.
Recuerdan?
Y porqué?
#balano
un dolor insoportable y una cirugía vergonzosa que arruinó la vida del muchacho, QEPD.
elpais.com/america-colomb….
Español
Sobre drogas y estrategias más sofisticadas en el manejo de mieloma múltiple. Anti BCMA, anti GPRC5d, ADC, anticuerpos bi-específicos, CAR-T cells. Ninguno disponible en Colombia, pero críticos para el entendimiento del panorama terapéutico de la enfermedad en el mundo - open.substack.com/pub/lemasobrec…

Español

Demis Hassabis says AI won’t just accelerate drug discovery.
It will replace the process entirely.
The pharmaceutical industry finds drugs the same way it has for decades.
Synthesize a compound. Test it on animals. Test it on humans. Wait years for approval. Hope the molecule doesn’t kill someone along the way.
Every step is physical.
Every step is slow.
Every step is expensive enough to make most diseases not worth curing.
Hassabis: “We’re focusing on solving the rest of the drug discovery process, which is a lot of chemistry, designing the compounds, checking it’s not toxic, and all the different properties you need for drugs to be safe.”
That sounds incremental.
It isn’t.
AlphaFold solved protein folding. Isomorphic Labs is now working through the rest of the chain.
Compound design. Toxicity screening. Safety profiling.
All computational. None of it requires a lab.
Hassabis: “I think we’ll have that whole drug design engine ready in the next five to 10 years.”
Not a tool that assists chemists.
A system that replaces the chemistry.
But designing the drug was never the bottleneck that killed people.
Clinical trials were.
A single drug takes over a decade to move from lab to patient. Most of that time isn’t science. It’s bureaucracy, logistics, and the blunt reality of testing molecules on living tissue one dose at a time.
Hassabis: “Simulating parts of the human metabolism, also stratifying patients to make sure that certain patients get exactly the right type of drug that’s suitable for their genomic makeup.”
Simulate the patient before you treat the patient.
Map individual DNA. Model personal metabolism. Test the drug on a digital replica before it touches a vein.
Not personalized medicine as a marketing phrase.
Personalized medicine as an engineering output.
The final wall is regulatory.
The FDA exists because humans make mistakes with molecules. Every approval gate was built to catch errors that cost lives.
The entire structure assumes the process is fallible.
What happens when the process stops being fallible.
Hassabis: “Perhaps like the animal testing is not needed anymore, maybe we can go up the dosage ladder quicker, because you can rely on these models.”
He’s not speculating. He’s describing a sequence.
AI-designed drugs enter the existing pipeline. A dozen compounds go through full traditional trials. Regulators collect data. They back-test model predictions against real outcomes.
Hassabis: “Then the government and the regulatory bodies see that and they have enough data to sort of back-test the predictions of those models.”
When the models prove more accurate than the trials they’re meant to replace, the trials become the bottleneck.
Not the science. The paperwork.
Animal testing shortened. Dosage ladders compressed. Entire stages of the pipeline collapsed into computation.
The drug doesn’t get discovered faster.
The drug gets discovered differently.
The laboratory moves from a building to a server.
The clinical trial moves from a hospital ward to a simulation.
The patient moves from a statistic to a genome.
Hassabis isn’t promising a cure for one disease.
He’s describing the architecture that makes curing disease an engineering problem with a known solution path.
The bottleneck was never biology.
It was the speed at which humans were allowed to solve it.
That speed limit is about to be revoked.
English
Drogas para mieloma múltiple - parte I: inhibidores de proteasoma, IMiDs, anti-CD38, dexametasona y agentes antiresrtivos. - open.substack.com/pub/lemasobrec…
Español

Quién me da una sola razón para votar por Cepeda ? Pero creíble por favor.
Español
@marlonjulianre2 @AndresFelArias @petrogustavo Uno refuta el argumento, no ataca a la persona (sutileza que como otras lo eluden, según puedo apreciar). No es por calidad moral la que habla, es la técnica. De eso sí sabe Arias.
Español

@AndresFelArias @petrogustavo CON TODO RESPETO, ESTAFADOR DE MIERDA USTED NO TIENE NINGUNA POTESTAD MORAL PARA VENIR A CRITICAR AL PRESIDENTE, CUANDO EN SU HABER SE DESTACA UNO DE LOS FRAUDES MAS GRANDES DE LA HISTORIA ECONOMICA DEL PAIS SU ETICA COMO "ECONOMISTA" VALE MONDA CARE VERGA....

Español

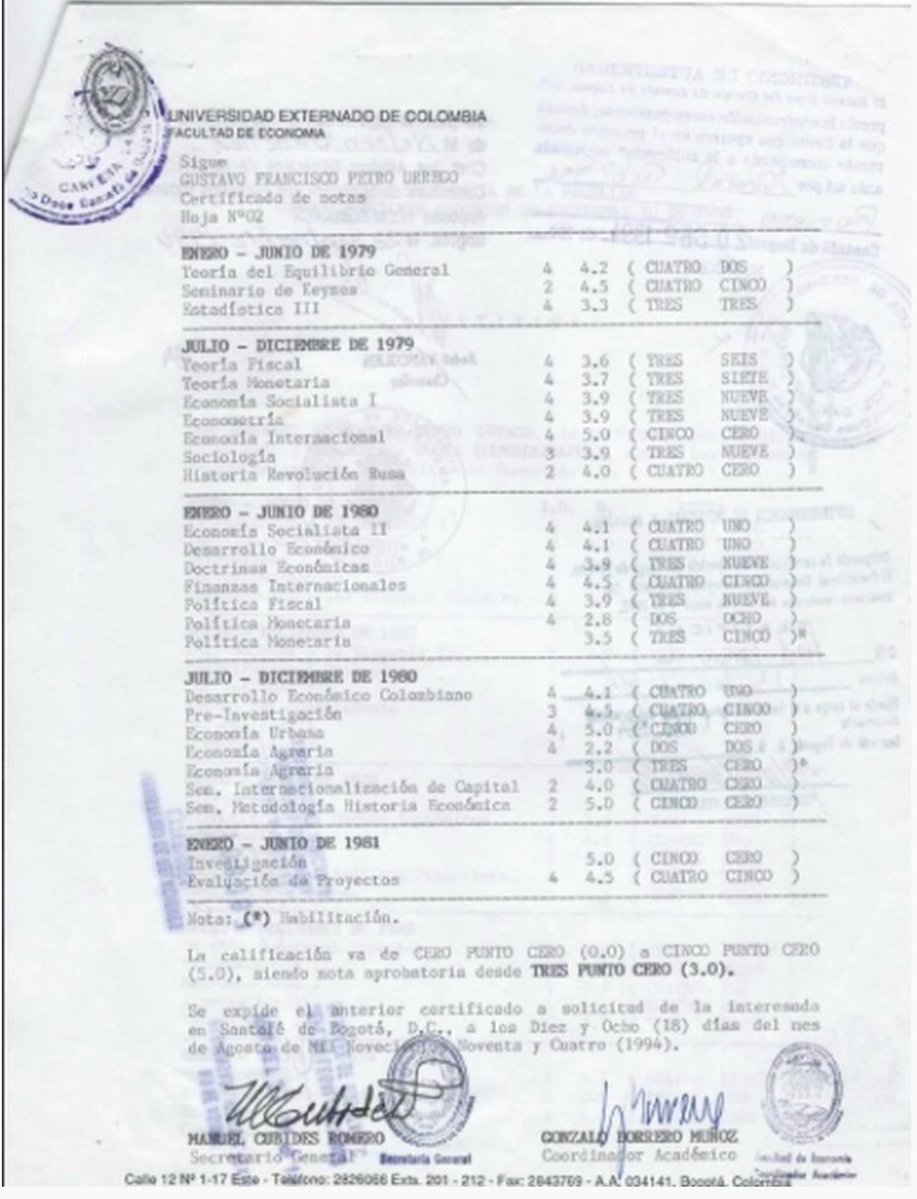
🎓 Señor Presidente @petrogustavo, con todo respeto: usted perdió Política Monetaria con 2.8 y Economía Agraria con 2.2 en el Externado.
📌Anoche, en su alocución, quedó claro que no habilitó ninguna de las dos. Un hilo. 🧵
Español
@Jhonny798253233 @AndresFelArias @petrogustavo Es la economía, estúpido. Si es Lunes, es Lunes... No importa quién lo diga. Y Arias lo dijo PERFECTO.
Español

@AndresFelArias @petrogustavo Jajajaja usted estuvo preso y ahora sale a dárselas de faro moral ,digamos que el encierro te hizo cambiar para pensar con honestidad para aportar al pueblo colombiano pero lo que vemos es que no aprendes delerror @petrogustavo cambio y demuestra queestá para el pueblo colombiano
Español
@philschmidtke Thank you, Dr. Schmidtke. You are the second person to point-out to me that IVUS merits more consideration.
English

@OncoNerd Not sure that IVUS is hype, and pressure gradients in small coronaries are very difficult to do accurately by any method
English
A mi hija le gusta la cardiología (como me gustó a mí por muchos años). Me encontré muchos artículos en el NEJM de cardiología de este mes (seguro que hubo un congreso, pensé). Le dije que le iba a hacer un resumen con Claude. Le dije: "in Browser, analyze the original papers recently published in the NEJM on cardiology. Create a 1 paragraph summary of each study" y me generó esto... - drive.google.com/file/d/18GUyAC… - Ya sé que el manejo sin anticoagulación es posible para la fibrilación auricular (en un estudio) y en el otro no. Los beta bloqueadores se pueden suspender al año del infarto al miocardio si la FEVI es mayor de 40%. El IVUS es pura bulla. Se puede definir en forma menos invasiva el gradiente de presión de las arterias coronarias intermedias para definir si se hace PCI. Hay droga para la cardiomiopatía hipertrófica (un anti miosina). El LDL colesterol hay que bajarlo por debajo de 55 en pacientes con aterosclerosis, y la fibrinolisis guiada por catheter es súper buena en embolismo pulmonar... Los demás, ya los olvidé. Algún cardiólogo misericordioso, están erradas mis conclusiones?
Español