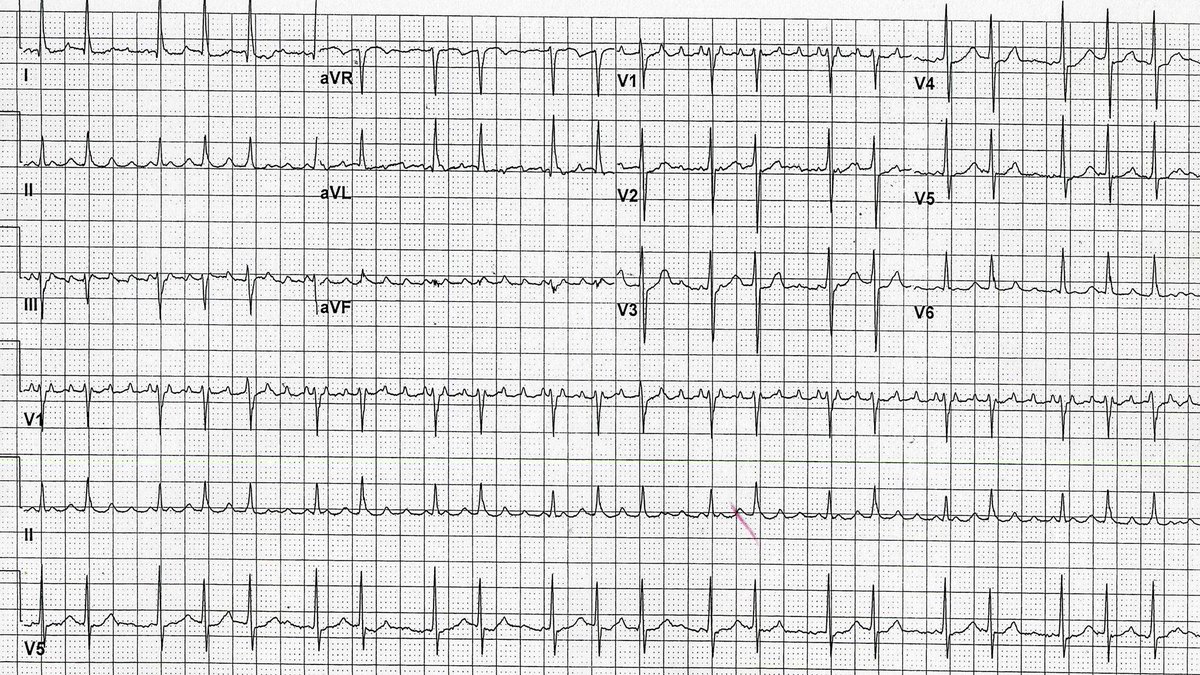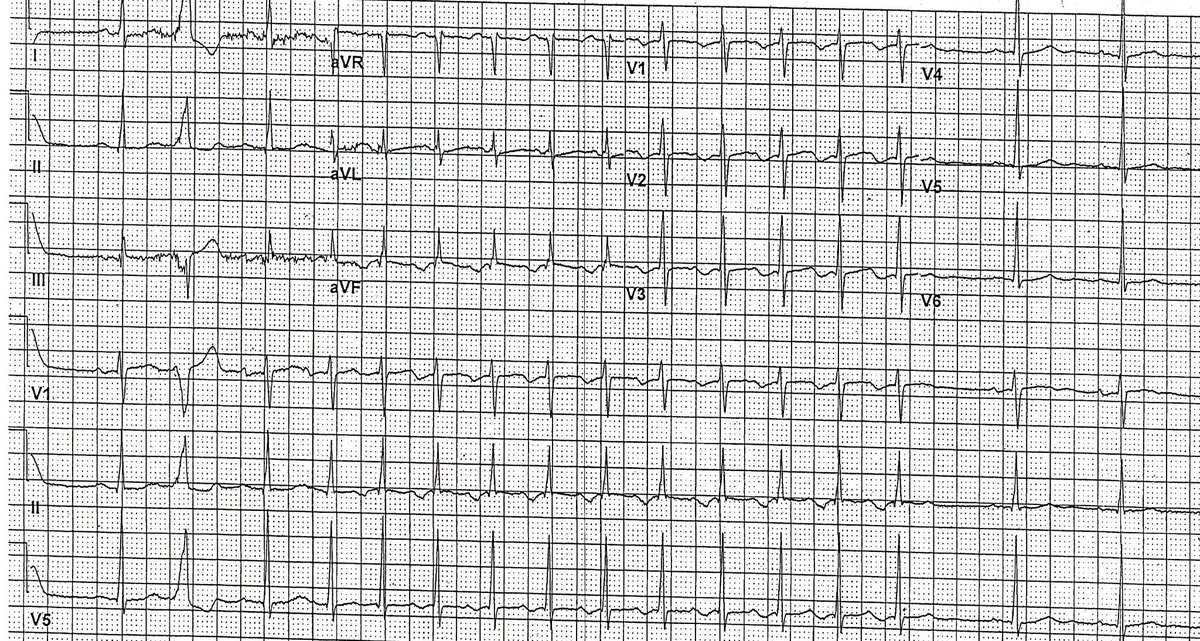
58 year old male with h/o hypertension, poorly treated, presents for routine pe. What does the ECG show? #PodridECGs #ECG #meded #cardiotwitter

English
Philip J Podrid MD
859 posts

@PPodrid
ECG Educator | Electrophysiologist | Professor @The_BMC | Alumni @BrighamFellows & @NYUMed | All tweets are my personal opinion 🩺