Sabitlenmiş Tweet

I think this is all I need @UlhasDr Thank you a million 🙇🏻♂️
Dr Ulhas Pandurangi@UlhasDr
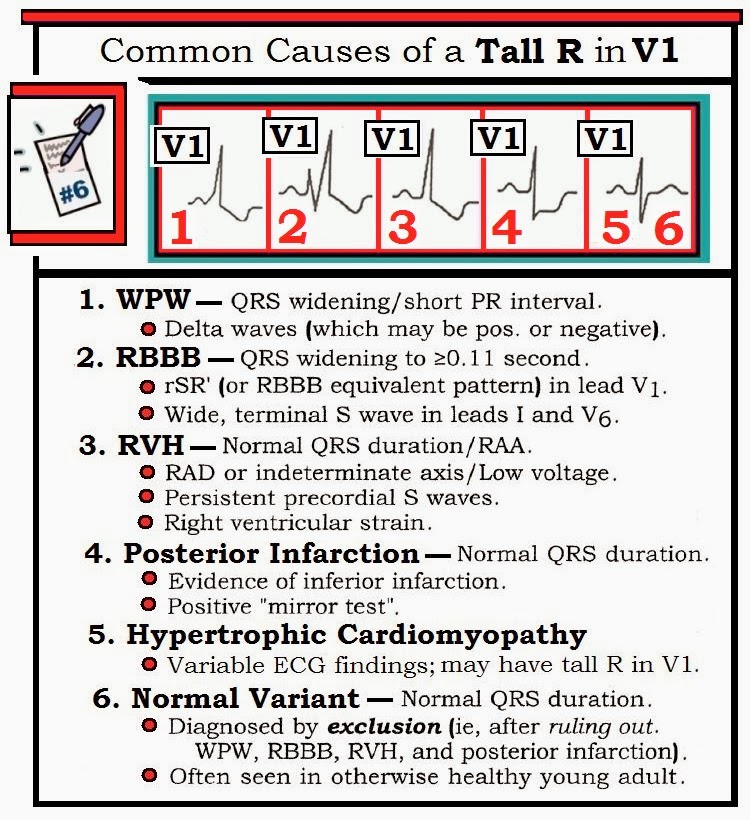
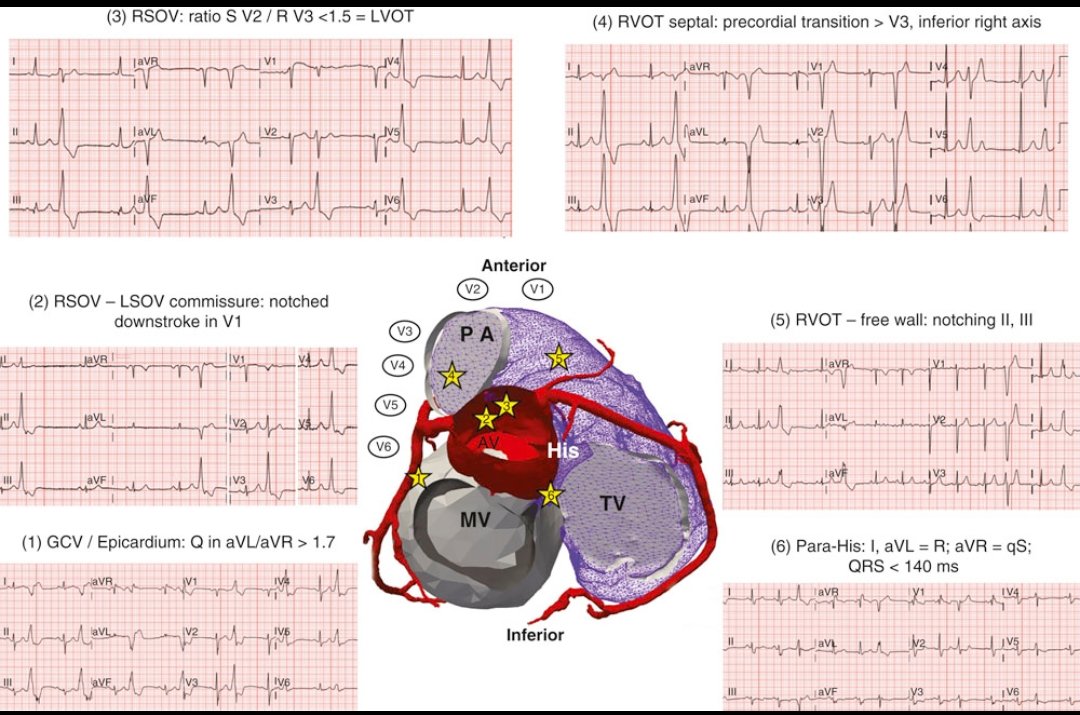
Let’s thread-together-ECG cheat sheets. Beginning from this masterpiece from @grepmeded #EPeeps @SchakrabartiEP @ecgrhythms @abhishek_mbbs @syamkumarmd @mahishasur @DCR_Dr @anunay_cardio @Hapa_EP @PaymardM @javadm20 @jeffrey_vinocur @narrowQRS @seshadribalaji6 @rdschaller
English