@NickHoopes_ I really hate clamshells. Most people cheat with their hip flexors, never actually works for the patients I see. Much prefer sit to stand and step ups
English
Derek Petit
3.1K posts
@PetitDerek
Papa & husband 🇨🇦 Physiatrist interested in everything MSK & EMG💪🩺 Deteriorating athlete & Fantasy sports junkie⛹♂🏈 Secret Sci-fi nerd🧬




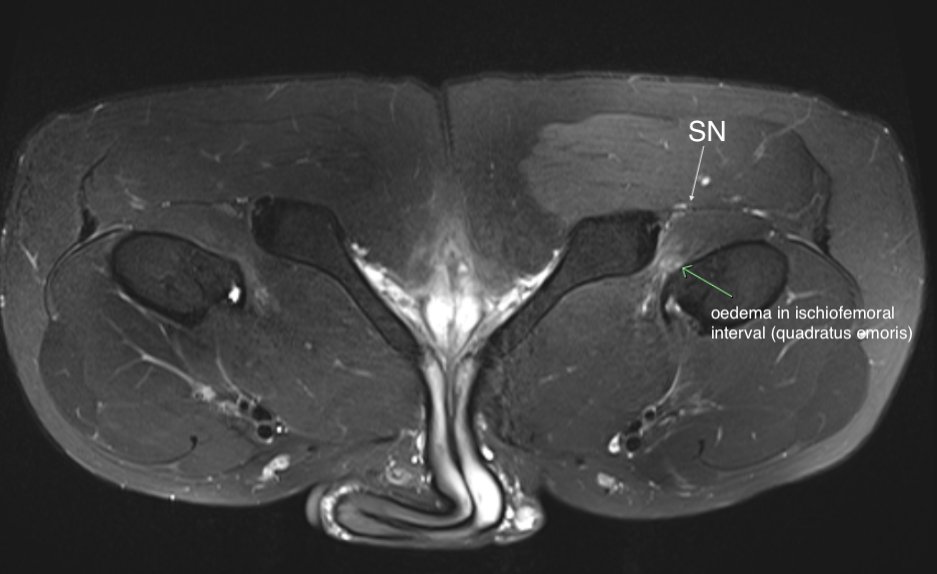


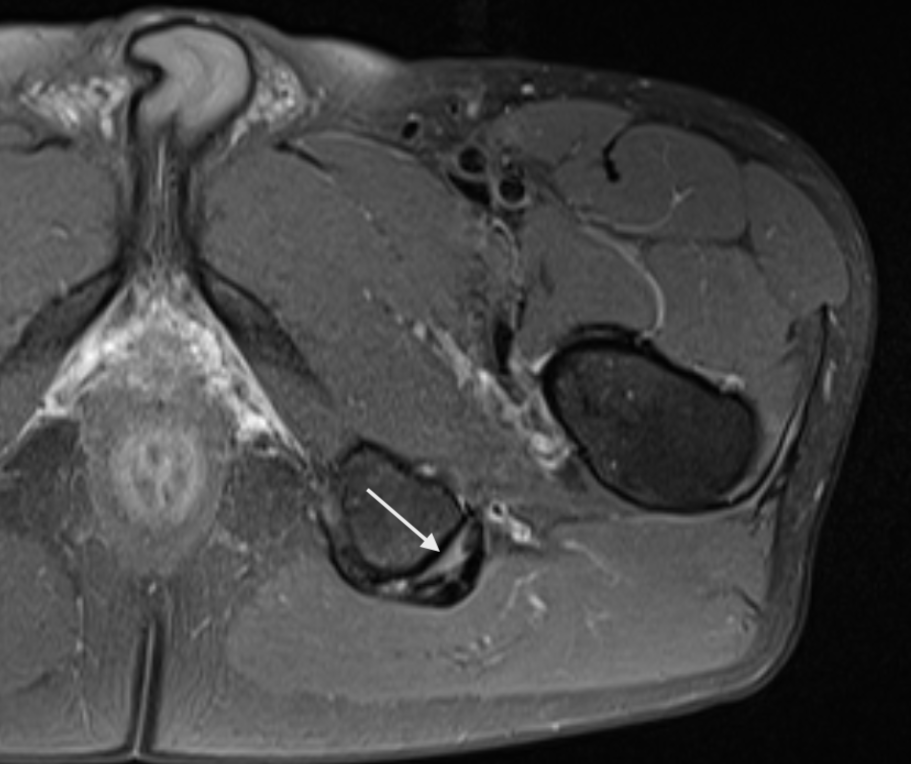
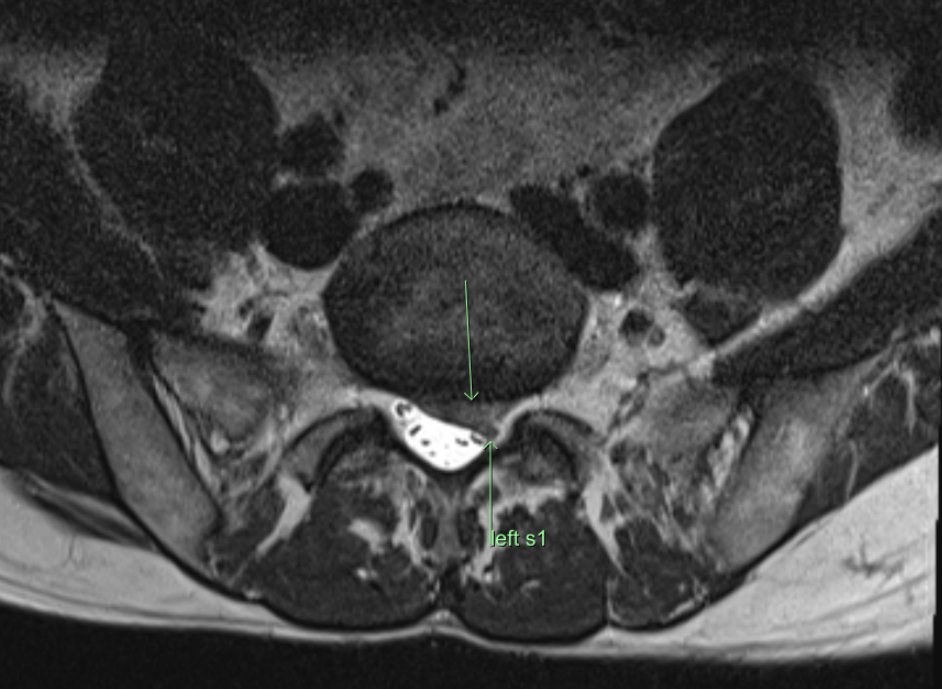
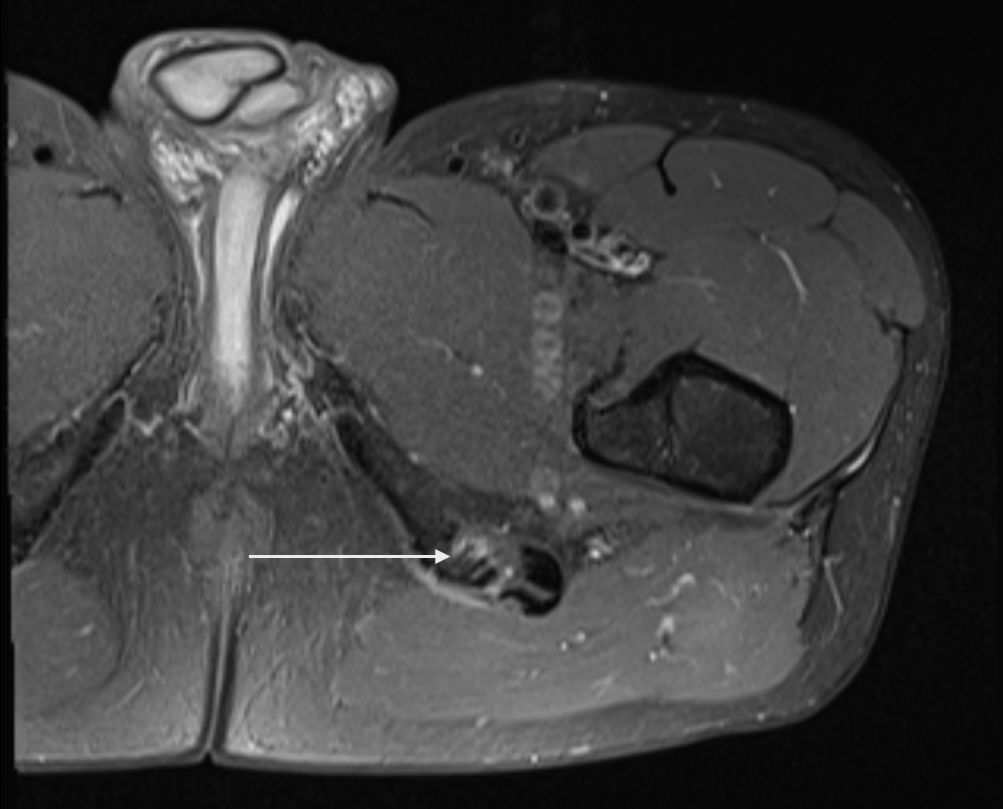

Consent✅ 1 year progressive severe (painless) L calf atrophy & weakness Medial bulk affected > lateral - see pic Affecting football performance Rolling over in bed onto R side - sudden 'spasms' in leg leg US - diffuse fatty atrophy of medial gastroc & soleus (vs R) EMG / NCS - severe L5 & S1 subacute chronic radiculopathy MRI - no herniated disc - but 5cm filum terminale lipoma (high signal on T1 seq, low on STIR). Also very low lying conus medullaris & tethered cord suggestive of spinal dysraphism (spina bifida occulta) Neurosurgical referral





Julia Hanes is headed to @paris2024 ‼️🎉 @aircanada Hanes officially meets the standard to qualify for the Paralympic Team after winning the F33 Shot Put final at #BellTrials24 👏 #FlyTheFlag #HautLeDrapeau